Actinic Keratosis: Diagnosis, Treatment, And Prevention Guide
Precancerous skin lesions from sun damage: symptoms, causes, diagnosis, treatment, and prevention strategies.

Actinic keratosis (AK), also known as solar keratosis, is a common precancerous skin condition caused by cumulative ultraviolet (UV) radiation exposure from the sun or tanning beds. These rough, scaly patches primarily affect sun-exposed areas and carry a risk of progressing to squamous cell carcinoma (SCC), a type of skin cancer, if untreated. Early detection and treatment are essential for prevention.
What is Actinic Keratosis?
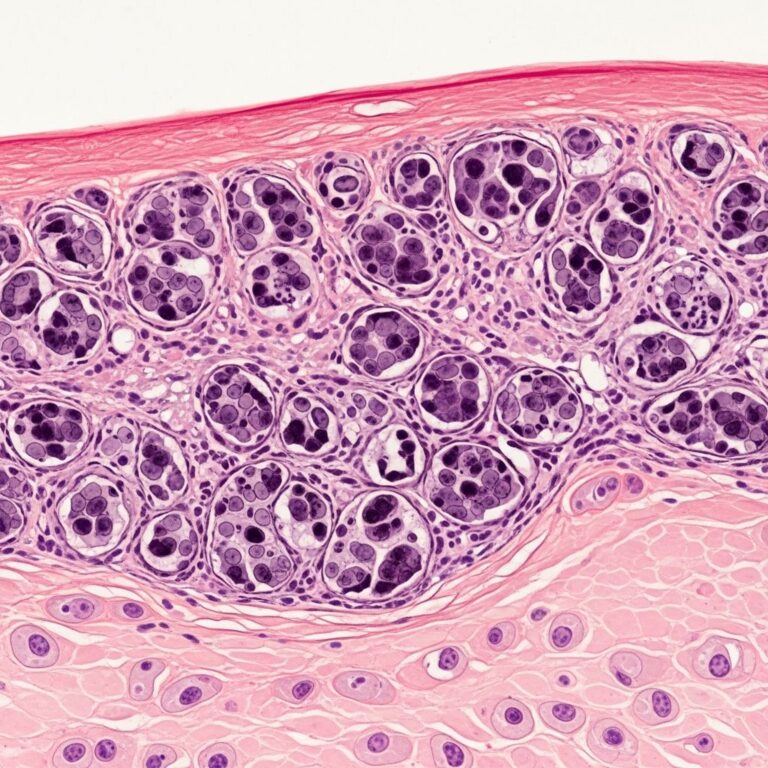
Actinic keratosis represents abnormal growth of keratinocytes, the main skin cells, due to DNA damage from UV rays. Lesions appear as small, rough, sandpaper-like spots less than 1 inch (2.5 cm) in diameter, often on the face, scalp, ears, neck, lips, forearms, and hands. While most AKs remain benign, about 5-10% may evolve into invasive SCC over time, emphasizing the need for vigilant monitoring.
AKs develop slowly over years of sun exposure, typically in fair-skinned individuals over age 40. They do not resolve spontaneously and require medical intervention to destroy precancerous cells and prevent malignancy.
Who Gets Actinic Keratosis?
Anyone with significant sun exposure can develop AK, but certain groups face higher risk:
- People over 40-50 years old, due to cumulative UV damage.
- Fair-skinned individuals (Fitzpatrick skin types I-II) with light hair (blonde/red), blue/green eyes, or freckling tendency.
- Those living in sunny climates or working outdoors (e.g., farmers, construction workers).
- History of severe sunburns, tanning bed use, or weakened immune systems (e.g., organ transplant recipients).
- Previous skin cancer or extensive sun exposure history.
Prevalence increases with age; up to 60% of fair-skinned adults over 40 in sunny regions may have subclinical AKs.
Symptoms of Actinic Keratosis
AK lesions vary in appearance but share common traits:
- Rough, dry, scaly patches feeling like sandpaper or abrasive surfaces.
- Flat to slightly raised bumps, sometimes with a stuck-on appearance.
- Colors: pink, red, brown, tan, or flesh-toned; may resemble age spots.
- Size: usually under 1 inch, but can grow thicker or wart-like.
- Symptoms: itching, burning, tenderness, bleeding, or crusting if irritated.
Multiple lesions often cluster (‘AK field’) in chronically sun-damaged skin. Subtle early lesions may only be visible after rubbing or stretching the skin.
Causes of Actinic Keratosis
The primary cause is long-term UV radiation exposure:
- UVB rays from midday sun (10 AM-4 PM) penetrate skin, mutating keratinocyte DNA via pyrimidine dimers.
- Cumulative dose matters more than single burns; indoor UV from tanning beds also contributes.
- Other factors: radiation therapy, certain chemicals (e.g., arsenic), or genetic predispositions like xeroderma pigmentosum.
Immunosuppression accelerates progression; transplant patients have 65-250 times higher risk.
Complications
Untreated AKs rarely regress and may thicken, ulcerate, or bleed, signaling progression. Key complication: transformation to SCC (0.025%-16% annual risk per lesion). SCC can invade locally or metastasize if advanced. Rare evolution to basal cell carcinoma or melanoma also occurs. Regular dermatologic surveillance prevents these outcomes.
Diagnosis of Actinic Keratosis
Diagnosis relies on clinical exam by a dermatologist:
- Visual/tactile inspection of suspicious lesions under dermoscopy for hyperkeratosis, vascular changes.
- Biopsy (shave or punch) if thick, indurated, ulcerated, or atypical to rule out SCC.
- Tools like confocal microscopy or AI-assisted imaging aid subclinical detection.
Dermoscopy reveals ‘strawberry pattern’ (white scaling over red base) or rosette vessels in hypertrophic AK.
Treatment of Actinic Keratosis
Treatment destroys visible and subclinical lesions to prevent progression. Options span lesion-directed (single spots) and field therapies (multiple/field cancerization):
Lesion-Directed Therapies
- Cryotherapy: Liquid nitrogen spray/freeze (-196°C) causes epidermal necrosis; most common, quick office procedure. Blisters form, then heal in 1-2 weeks. Hypopigmentation/hyperpigmentation risk.
- Curettage/Curettage-Electrodessication: Scrape with curette ± electric current to destroy base. For hypertrophic lesions.
- Laser Ablation: CO2 or Er:YAG lasers vaporize tissue precisely; good for thick lesions.
Field Therapies (for Multiple Lesions)
- Topical Agents:
- 5-Fluorouracil (5-FU) 5% cream: Twice daily 2-4 weeks; induces inflammation (erosion phase).
- Imiquimod 5%/3.75% cream: Immune modulator; weekly 2-16 weeks.
- Diclofenac 3% gel: NSAID inhibiting COX-2; 60-90 days.
- Ingenol mebutate 0.015%/0.05% gel: 2-3 days; induces cell death.
- Tirbanibulin 1% ointment: 5 days; microtubule inhibitor.
- Photodynamic Therapy (PDT): Apply aminolevulinic acid (ALA), incubate 1-3 hours, then blue/red light activates protoporphyrin IX to kill cells. Effective for fields; cosmetic outcome good.
- Chemical Peels: Trichloroacetic acid (TCA) or medium-depth peels remove epidermis.
Choice depends on lesion number, size, location, patient tolerance. Combination therapies optimize clearance (80-95%).
| Treatment | Indications | Duration | Side Effects |
|---|---|---|---|
| Cryotherapy | Isolated lesions | Seconds | Blistering, pigment changes |
| 5-FU Cream | Field therapy | 2-4 weeks | Redness, erosion, pain |
| PDT | Multiple lesions | 1 session | Burning, crusting |
| Imiquimod | Field, high-risk | 2-16 weeks | Flu-like symptoms |
Prevention of Actinic Keratosis
Primary prevention targets UV avoidance:
- Apply broad-spectrum SPF 50+ sunscreen daily, reapply every 2 hours.
- Wear UPF 50+ clothing, wide-brim hats, sunglasses.
- Seek shade 10 AM-4 PM; avoid tanning beds.
- Self-exams monthly; annual dermatologist skin checks for high-risk.
- Antioxidants (e.g., nicotinamide 500mg BID) reduce new AKs by 23%.
Outlook
With treatment, 75-95% clearance rates; recurrence common (40-60% in 1 year) due to ongoing UV damage. Lifelong sun protection and surveillance mitigate risk. Most patients manage AK effectively without progression to cancer.
Frequently Asked Questions (FAQs)
Q: Do actinic keratoses go away on their own?
A: No, AKs do not resolve spontaneously and require treatment to prevent progression.
Q: Is actinic keratosis cancerous?
A: AK is precancerous; untreated, 5-10% may become SCC.
Q: How is cryotherapy performed?
A: Liquid nitrogen freezes the lesion for seconds; a blister forms and peels off in 7-14 days.
Q: Can I treat AK at home?
A: No, prescription topicals require dermatologist oversight; self-treatment risks incomplete clearance.
Q: How often should I see a dermatologist?
A: High-risk patients: every 6-12 months for full skin exams.
References
- Actinic Keratosis: Symptoms and Treatment — Creedmoor Skin Surgery Center. 2023. https://www.creedmoorskinsurgerycenter.com/conditions/actinic-keratosis
- Actinic Keratosis Symptoms and Treatment Options — SJPP Dermatology. 2024. https://www.sjpp.org/dermatology/conditions/bumps-spots/actinic-keratosis/
- Actinic Keratosis Symptoms & Treatment — Aurora Health Care. 2024. https://www.aurorahealthcare.org/services/dermatology/actinic-keratosis
- Actinic Keratosis Treatment, Symptoms, Causes — Spectrum Dermatology. 2023. https://www.specdermatl.com/actinic-keratosis/
- Actinic Keratosis — Yuma Dermatology. 2024. https://www.yumadermatology.com/services/actinic-keratosis/
- Actinic Keratosis – Symptoms & Causes — Mayo Clinic. 2025-01-15. https://www.mayoclinic.org/diseases-conditions/actinic-keratosis/symptoms-causes/syc-20354969
Similar Articles






Read full bio of Sneha Tete