Anisocoria: Unequal Pupil Size Causes & When to Seek Care
Understanding anisocoria: Learn what causes unequal pupils and when you need emergency care.

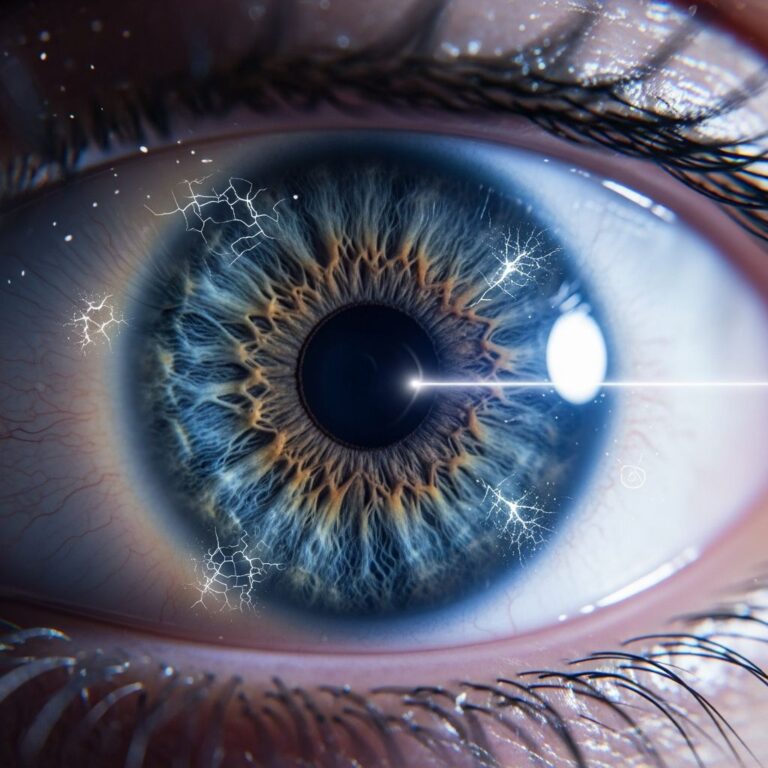
Anisocoria is a condition characterized by pupils of unequal sizes, where one pupil appears noticeably larger than the other. This clinical sign occurs in approximately 20% of the population, making it relatively common. While many cases are benign and require no treatment, anisocoria can occasionally indicate serious underlying medical conditions ranging from minor trauma to potentially life-threatening pathologies. Understanding the causes, how to identify problematic anisocoria, and when to seek emergency care is essential for proper health management.
What Is Anisocoria?
Anisocoria literally refers to unequal pupils. The condition is defined when the difference in pupil size exceeds 0.5 millimeters. The pupils are controlled by the autonomic nervous system, which regulates their constriction and dilation in response to light, emotions, and various physical conditions. When this system functions improperly or when other factors interfere with normal pupil regulation, anisocoria results.
The condition can be classified into three main categories based on pupillary reaction to light: physiologic anisocoria (normal variation), a pathologically large pupil, or a pathologically small pupil. This classification system helps healthcare providers determine the underlying cause and appropriate management strategy.
Types and Prevalence of Anisocoria
Physiologic anisocoria, also called simple or essential anisocoria, represents the most common form of the condition. It is estimated to be present in 10-30% of the population and is not associated with any disease process. Physiologic anisocoria typically involves a pupillary size difference of less than or equal to 1 millimeter and can be persistent, self-limiting, unilateral, or of variable laterality. This benign form requires no treatment and no medical intervention beyond proper documentation to prevent unnecessary future medical workups.
In contrast, pathologic anisocoria indicates an underlying medical condition requiring investigation and potential treatment. Determining whether anisocoria is acute or chronic represents an important diagnostic step, as this distinction helps guide the urgency and type of evaluation needed.
Causes of Anisocoria
Benign Causes
Many causes of anisocoria are entirely benign and self-resolving. Physiologic anisocoria accounts for the majority of cases and requires only observation. Previous eye trauma or surgery can result in anisocoria that may resolve over time or remain permanent. Certain medications, particularly eye drops used during ophthalmologic examinations or for treating eye conditions, can cause temporary anisocoria that resolves as the medication wears off.
Medication-Related Causes
Both systemic and topical medications can cause anisocoria through various mechanisms. Anticholinergic medications inhibit parasympathetic signaling at the neuromuscular junction of the pupillary sphincter and ciliary muscles, leading to mydriasis (pupil dilation). Examples include scopolamine patches, belladonna, Jimson weed, and angel’s trumpet. Sympathomimetic drugs can also cause anisocoria by affecting the sympathetic nervous system’s regulation of pupil size. Direct inoculation with these agents—whether through accidental exposure, occupational contact, or intentional administration—can result in notable pupillary changes.
Horner Syndrome
Horner syndrome causes a pathologically small pupil and represents one of the more significant causes of anisocoria requiring evaluation. This condition results from disruption of the sympathetic nerve pathway controlling pupil dilation. Horner syndrome can be caused by central lesions, preganglionic lesions, or postganglionic lesions along the sympathetic pathway. Associated symptoms may include ptosis (drooping eyelid), anhidrosis (decreased sweating), and facial flushing. Concerning causes of Horner syndrome include carotid artery dissection, which accounts for 2.5% of strokes, and Pancoast lung tumors. When Horner syndrome appears with pain, particularly in the neck or head, it warrants emergency evaluation for possible carotid artery dissection.
Third Nerve Palsy
Oculomotor (third cranial) nerve palsy causes a pathologically large pupil and represents a potentially life-threatening cause of anisocoria. This condition results in significant ptosis of the affected upper eyelid and characteristic positioning of the eye described as “down and out” due to unopposed action of the lateral rectus and superior oblique muscles. A critical concern is that a ruptured aneurysm can cause third nerve palsy and carries a very poor prognosis, with only approximately 50% of patients surviving six months after a ruptured aneurysm. Even pure oculomotor dysfunction without pupillary involvement can represent the early presentation of an aneurysm in up to 14% of cases, warranting thorough investigation.
Adie Tonic Pupil
Adie tonic pupil is a benign condition causing a pathologically large pupil. The affected pupil dilates poorly to light but reacts to accommodation (focusing). This condition typically occurs in young adults and is more common in women. Adie tonic pupil requires only observation and documentation, as it is self-limiting and poses no health risk.
Other Causes
Additional causes of anisocoria include uveitis (inflammation of the uveal tract), iris-lens epithelial (ICE) syndrome, neovascularization of the iris, headaches, and trauma. Each of these conditions may require specific treatment addressing the underlying pathology rather than the anisocoria itself.
Diagnostic Evaluation
Clinical History
Proper evaluation of anisocoria begins with focused history-taking. Key information includes recent head, neck, or eye trauma; past ocular procedures; use of eyedrops or other topical medications; presence of neurologic symptoms; and timeline of symptom onset. Determining whether anisocoria is new or chronic is essential, and patients should be asked to review old photographs from social media or driver’s licenses, as they often do not notice gradual or chronic changes in pupil size.
Physical Examination
A comprehensive ocular assessment forms the foundation of anisocoria evaluation. This includes measurement of visual acuity, assessment of visual fields, evaluation of extraocular eye movements, and testing for an afferent pupillary defect (APD). The examiner must observe pupil reactions to light and accommodation in both bright and dim lighting conditions. Measurement of the degree of anisocoria and documentation of which pupil is larger represents critical information for diagnosis and tracking progression or resolution.
Pharmacologic Testing
When diagnostic uncertainty exists regarding the cause of anisocoria, pharmacologic testing using eye drops can assist in differentiation. Cocaine testing, using 4-10% cocaine solutions, helps identify Horner syndrome by blocking norepinephrine reuptake; in Horner syndrome, the affected pupil dilates minimally or not at all, with post-drop anisocoria of 0.8 millimeters or more considered positive. Apraclonidine, a selective alpha-2 adrenergic agonist, relies on denervation supersensitivity and shows different findings, with the abnormal eyelid rising and the pupil dilating to reverse the deficit within 30-45 minutes. However, pharmacologic testing has limitations and should not be relied upon exclusively; thorough history and physical examination remain the cornerstone of evaluation.
Imaging Studies
Acute onset anisocoria concerning for compressive third nerve palsy or Horner syndrome warrants immediate imaging. Computed tomography angiography (CTA) of the head and neck is the indicated study to evaluate for aneurysm or vascular abnormalities. Patients with signs suggesting carotid artery dissection require emergency imaging and vascular surgery consultation.
When to Seek Emergency Care
Emergency evaluation is essential if anisocoria appears with any of the following warning signs: sudden severe headache, vision loss, neurological symptoms, blood in sputum, sudden blurring of vision, or signs of stroke. Acute onset anisocoria associated with pain, particularly in the neck, should be evaluated immediately for possible carotid artery dissection. Any anisocoria accompanied by significant ptosis, eye deviation, or neurologic deficits requires urgent assessment in an emergency department.
Treatment and Management
Treatment of anisocoria depends entirely on the underlying condition causing the condition. Most causes of anisocoria require only observation and proper documentation. Physiologic anisocoria and Adie tonic pupil simply require observation to prevent unnecessary medical workup in the future. Anisocoria due to medication typically resolves over time as the medication is cleared from the system. Anisocoria resulting from trauma may remain permanent but may also improve with time.
Conditions such as uveitis, ICE syndrome, and neovascularization of the iris require treatment of the underlying pathology. Referral to a neuro-ophthalmologist, ophthalmologist, or neurologist may be warranted in cases that do not resolve or when serious pathology is suspected. Surgical management is rarely necessary for anisocoria itself, though underlying conditions may require intervention.
Horner syndrome associated with pain requires emergency recognition and treatment of the underlying cause. Ruptured aneurysms causing third nerve palsy necessitate immediate neurosurgical consultation and specialized intensive care management.
Prognosis
The prognosis of anisocoria depends entirely on the causative factor. For most benign causes, prognosis is excellent with complete resolution or stable nonprogressive condition. However, certain serious causes carry poor prognosis. Ruptured aneurysms causing third nerve palsy have a very poor prognosis, with only approximately 50% of patients surviving six months. Horner syndrome caused by carotid artery dissection carries significant stroke risk, while Pancoast lung tumors require oncologic management with variable outcomes depending on disease stage.
Patient Education and Prevention
Patients should be educated that anisocoria is a clinical sign they may not be able to identify themselves. However, they should understand that sudden severe headache, blood in sputum, or sudden blurring of vision associated with anisocoria warrants immediate medical evaluation. Patients with known anisocoria should have photographs or documentation of baseline pupil appearance to help distinguish chronic from acute changes. Awareness of risk factors, including trauma, medications, and neurologic symptoms, helps patients recognize when professional evaluation is needed.
Frequently Asked Questions About Anisocoria
Q: Is anisocoria always a sign of a serious condition?
A: No. Physiologic anisocoria affects 10-30% of the population and is completely benign, requiring no treatment. However, new-onset anisocoria or anisocoria accompanied by other symptoms should be evaluated by a healthcare provider to exclude serious underlying conditions.
Q: Can medications cause anisocoria?
A: Yes. Both topical eye drops and systemic medications can cause temporary anisocoria. Anticholinergic and sympathomimetic medications are common culprits. Medication-related anisocoria typically resolves as the drug is cleared from the system.
Q: What should I do if I notice sudden unequal pupils?
A: Contact your healthcare provider or visit an urgent care center. If the change is accompanied by headache, vision loss, difficulty moving your eyes, drooping eyelid, or any neurologic symptoms, seek emergency care immediately.
Q: How is anisocoria diagnosed?
A: Diagnosis begins with patient history and physical examination, including pupil measurement and assessment of light reactions. Depending on findings, pharmacologic testing with special eye drops or imaging studies such as CTA may be performed to identify the underlying cause.
Q: Can anisocoria be treated?
A: Treatment depends on the underlying cause. Benign anisocoria requires only observation. Medication-related anisocoria resolves when the medication is discontinued or metabolized. Other causes require treatment of the underlying condition.
References
- Anisocoria — National Center for Biotechnology Information (NCBI) StatPearls. 2024. https://www.ncbi.nlm.nih.gov/books/NBK470384/
- Anisocoria in the Emergency Department: Pathophysiology, Evaluation, and Management — EM Docs Emergency Medicine Education. 2024. https://www.emdocs.net/anisocoria-in-the-ed-pathophysiology-evaluation-and-management/
- Dilated Pupils (Mydriasis): What Is It, Causes & What It Looks Like — Cleveland Clinic. 2024. https://my.clevelandclinic.org/health/symptoms/22238-dilated-pupils
- Unequal Pupil Size (Anisocoria): Causes & When to Worry — Cleveland Clinic Reference. 2024. https://smart.dhgate.com/unequal-pupil-size-anisocoria-causes-when-to-worry-5/
- The Prevalence of Simple Anisocoria — American Journal of Ophthalmology. 1987;104(1):69-73. https://www.ajopht.org/
- Horner Syndrome: Diagnostic Approach and Management — Cleveland Clinic Journal of Medicine. 1991;58(3):229-234. https://www.ccjm.org/
- One Pupil Dilated? Understanding Anisocoria Causes & Symptoms — Clinical Reference Resource. 2024. https://smart.dhgate.com/one-pupil-dilated-understanding-anisocoria-causes-symptoms/
Similar Articles






Read full bio of Sneha Tete