Annular Erythema: Causes, Diagnosis, And Treatment
Chronic ring-shaped red skin rashes: causes, diagnosis, and management strategies.

Annular erythema refers to a group of chronic skin conditions characterized by ring-shaped (annular), arc-like, or polycyclic erythematous eruptions that slowly expand with central clearing. These rashes typically begin as small pink-red papules or spots that enlarge peripherally at 2–5 mm per day, forming rings up to 6–8 cm in diameter, often with a fine trailing scale on the inner edge.
Who gets annular erythema?
Annular erythema can affect individuals of any age, from infants to the elderly, with no strong gender predilection reported. It most commonly appears on the thighs and legs but can involve the face, trunk, arms, and upper extremities; palms and soles are typically spared. Lesions are usually asymptomatic but may cause mild itching or stinging in some cases.
What causes annular erythema?
The exact cause of annular erythema remains idiopathic in most instances, but it is classified as a reactive erythema often triggered by hypersensitivity responses to various stimuli. Associated factors include:
- Infections: Such as dermatophytosis (tinea), herpes zoster, or tuberculosis.
- Drugs: New medications, including antimalarials, gold, or vaccines.
- Malignancies: Hodgkin lymphoma, other cancers (e.g., stomach, breast, ovary), sometimes preceding diagnosis by up to 2 years.
- Autoimmune/Connective Tissue Diseases: Lupus erythematosus, dermatomyositis, or Sjögren syndrome.
- Other: Endocrine disorders, pregnancy, or idiopathically.
In erythema annulare centrifugum (EAC), a key subtype, superficial and deep forms exist, with the deep type showing more indurated borders without prominent scale.
What are the clinical features of annular erythema?
Lesions start as small erythematous papules that expand centrifugally, clearing centrally to form annular, arciform, polycyclic, serpiginous, or gyrate patterns. Key features include:
- Advancing outer red edge (3–6 mm wide), often raised or indurated in deep forms.
- Trailing scale: Fine desquamation along the inner margin, classic for superficial EAC.
- Size: Millimeters to over 10 cm; growth rate 2–5 mm/day.
- Color: Pink to red, with possible central pallor or hyperpigmentation post-resolution.
- Symptoms: Usually none; pruritus in 50–70% of cases; rare vesiculation.
Lesions persist weeks to months, may recur, and rarely scar, though postinflammatory hyperpigmentation can occur. Nail changes like white toenail bands are occasional.
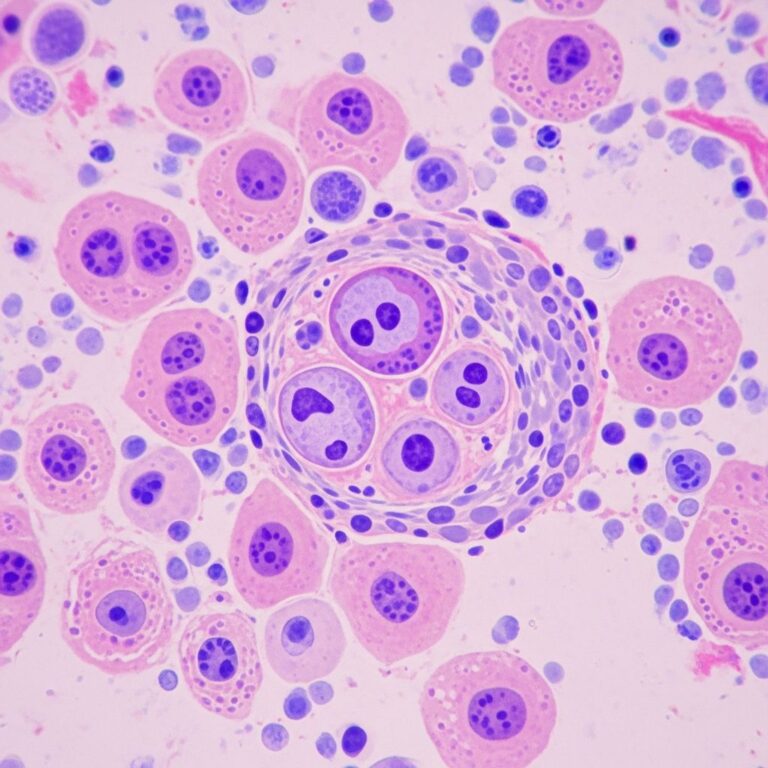
Pathophysiology
Histologically, annular erythema shows a perivascular ‘coat-sleeve’ lymphocytic infiltrate in superficial (upper dermis) or deep (around vessels to subcutis) plexuses. This reactive pattern suggests immune-mediated responses to antigens, without epidermal changes beyond trailing scale.
How is annular erythema diagnosed?
Diagnosis is primarily clinical, especially with trailing scale and centrifugal expansion. Confirmation involves:
- Skin biopsy: Reveals diagnostic lymphocytic perivascular infiltrate.
- Investigations: To identify underlying causes—complete blood count, ESR, fungal scrapings, cultures, ANA, malignancy screens (e.g., imaging if paraneoplastic suspected).
No systemic symptoms usually, but screen for fever, night sweats if present.
Differential diagnosis of annular erythema
Numerous conditions mimic annular erythema due to ring-like morphology. Key differentials include:
| Condition | Key Distinguishing Features |
|---|---|
| Tinea corporis | Scaly, itchy annular plaques; KOH+ hyphae; responds to antifungals. |
| Granuloma annulare | Firm, smooth papules; no scale; histo shows palisading granulomas. |
| Erythema multiforme | Target lesions on acral sites; mucosal involvement; acute. |
| Subacute cutaneous lupus | Polycyclic with hypopigmentation/telangiectasia; anti-Ro+. |
| Nummular eczema | Coin-shaped vesicular plaques; dry skin history. |
| Erythema marginatum | Evanescent, non-scaly; rheumatic fever link; neutrophilic. |
| Erythema migrans | Tick bite history; Lyme disease; single expanding lesion. |
| Secondary syphilis | Non-pruritic scaly plaques; RPR+; palm/sole involvement. |
Other: Psoriasis, pityriasis rosea, sarcoidosis, cutaneous metastases.
What is the treatment for annular erythema?
Most cases are self-limited (average 11 months), requiring no therapy beyond reassurance. Treat underlying causes if identified (e.g., antifungals for tinea, antineoplastics for malignancy). Symptomatic options:
- Topical corticosteroids: Potent agents (e.g., clobetasol) reduce inflammation/itch.
- Topical calcineurin inhibitors: Tacrolimus for steroid-sparing.
- Systemic: Hydroxychloroquine, indomethacin, or UVB phototherapy for refractory cases.
- Avoid triggers: Discontinue suspect drugs.
What is the outcome for annular erythema?
Lesions resolve spontaneously without scarring, though hyperpigmentation may linger. Recurrences are common; chronic cases last years. Prognosis improves with cause identification/treatment; monitor for malignancy.
Prevention
No specific prevention exists for idiopathic forms. Prompt treatment of infections/drugs and regular malignancy screening in persistent cases may help.
Frequently Asked Questions (FAQs)
What does annular erythema look like?
Ring-shaped red rashes with central clearing and possible inner trailing scale, expanding slowly on limbs.
Is annular erythema contagious?
No, it is a reactive/non-infectious process unless secondary to tinea.
Does annular erythema indicate cancer?
Sometimes, especially EAC preceding lymphoma; investigate persistent cases.
How long does annular erythema last?
Weeks to years; average 11 months, self-resolving in most.
Can annular erythema be cured?
Treat underlying cause; idiopathic cases managed symptomatically, often resolve.
References
- Erythema annulare centrifugum – DermNet — DermNet NZ. 2023. https://dermnetnz.org/topics/erythema-annulare-centrifugum
- Erythema Annulare Centrifugum — Patient.info. 2023-05-18. https://patient.info/doctor/dermatology/erythema-annulare-centrifugum
- Erythema Annulare Centrifugum – StatPearls — NCBI Bookshelf (NIH). 2023-07-17. https://www.ncbi.nlm.nih.gov/books/NBK482494/
- Annular erythema – DermNet — DermNet NZ. 2023. https://dermnetnz.org/topics/annular-erythema
- Annular Lesions: Diagnosis and Treatment — American Academy of Family Physicians (AAFP). 2018-09-01. https://www.aafp.org/pubs/afp/issues/2018/0901/p283.html
Similar Articles






Read full bio of Sneha Tete