Auricle Pseudocyst: Pathology, Diagnosis & Treatment
Comprehensive guide to auricular pseudocyst pathology, clinical features, and evidence-based treatment approaches.

Auricle Pseudocyst: Understanding the Pathology and Clinical Presentation
Auricular pseudocyst, also referred to as endochondral pseudocyst, cystic chondromalacia, or intracartilaginous auricular seroma cyst, represents a benign, asymptomatic cutaneous lesion that develops within the cartilaginous structure of the upper ear. This condition is characterized by the spontaneous accumulation of viscous fluid within an intracartilaginous cavity, typically presenting as a soft, fluctuant swelling that progressively firms over time. Understanding the pathological nature of this condition is essential for accurate diagnosis and appropriate management, as it remains relatively uncommon in general dermatological practice.
Clinical Features and Presentation
Auricular pseudocysts present as nontender, noninflammatory cystic lesions that develop gradually over a 4- to 12-week period, with diameters typically ranging from 1 to 5 cm. The condition most commonly manifests as a unilateral swelling on the upper portion of the auricle, particularly affecting the region encompassing the helix, antihelix, or scaphoid fossa, with the right ear being more frequently involved. However, bilateral presentations have been documented, though they remain relatively uncommon.
The characteristic appearance includes:
- Flesh-colored or skin-colored cystic lesion
- Smooth, fluctuant surface tension
- Normal overlying skin without erythema or warmth
- Gradual progression from soft to firmer consistency
- Absence of tenderness or pain on palpation
The lesion contains a viscous substance resembling olive oil with a straw-yellow hue, though serous or serosanguinous fluid may occasionally be present. The condition predominantly affects young adult males, with some studies suggesting a higher prevalence among Asian populations.
Etiology and Pathogenesis
The exact etiology of auricular pseudocyst remains incompletely understood, though multiple mechanisms have been proposed. While the condition can develop spontaneously without any identifiable precipitating factor, prior traumatic injury to the ear is recognized as a significant initiating factor in a substantial proportion of cases. The trauma theory suggests that mechanical injury causes separation of tissue planes within the auricular cartilage, leading to subsequent accumulation of fluid in the created space.
Alternative etiological hypotheses include:
- Cartilage fragmentation resulting from minor trauma
- Congenital embryonic dysplasia of cartilaginous tissue
- Inflammatory response triggered by unknown mechanisms
- Primary cartilage degeneration without apparent external cause
The lack of clear understanding regarding pathogenesis underscores the need for continued investigation into the biological mechanisms underlying pseudocyst formation.
Histopathological Features and Findings
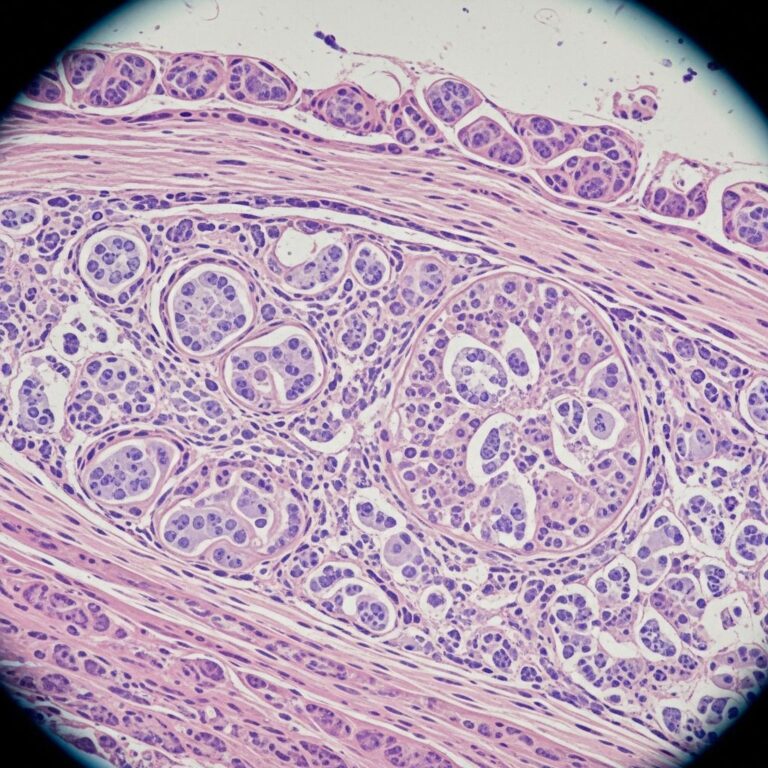
Histopathological examination provides crucial diagnostic confirmation and reveals the distinguishing characteristics of auricular pseudocysts. The defining histological feature is the presence of an intracartilaginous cyst devoid of epithelial lining, which accounts for the term “pseudocyst” rather than true cyst. This absence of epithelial lining differentiates pseudocysts from genuine cystic lesions and is pathognomonic for this condition.
Key histopathological observations include:
- Fibrous, cartilaginous, and granulation tissue lining without epithelial component
- Hyalinizing degeneration of surrounding cartilage
- Perivascular mononuclear infiltrates of lymphocytes in connective tissue superficial to anterior cartilage
- Early lesions: fibrosed cartilage surrounding cystic space
- Advanced lesions: necrosis and dissolution of cartilage with intracavity granulation tissue
- Extensive intracartilaginous fibrosis in later stages
The consistent presence of perivascular inflammatory infiltrates across all examined specimens suggests that inflammatory mechanisms play a crucial role in the pathogenesis of auricular pseudocysts. This inflammatory component may represent the tissue’s response to cartilage degeneration or primary inflammatory injury, though the precise trigger remains undefined.
Diagnosis and Diagnostic Approach
Diagnosis of auricular pseudocyst is typically established through a combination of clinical assessment and supportive investigations. The diagnostic approach includes:
Clinical History and Physical Examination
A thorough patient history documenting the onset of swelling, presence or absence of preceding trauma, and symptom progression is essential. Physical examination should document the location, size, consistency, and any associated symptoms. The characteristic appearance of a nontender, fluctuant swelling in the upper auricle with normal overlying skin provides strong clinical suspicion for pseudocyst diagnosis.
Histopathological Analysis
When diagnosis remains uncertain clinically, histopathological examination provides definitive confirmation. Tissue specimens obtained through aspiration or biopsy reveal the pathognomonic features of intracartilaginous cyst without epithelial lining. This analysis eliminates diagnostic uncertainty and excludes mimicking conditions.
Differential Diagnosis
Several conditions must be differentiated from auricular pseudocyst due to similar clinical presentation:
| Differential Diagnosis | Distinguishing Features |
|---|---|
| Subperichondrial Hematoma | History of significant trauma, acute presentation, dark discoloration, associated pain |
| Chondrodermatitis Helicis | Painful lesion, ulceration of overlying skin, located on helix rim, exudative drainage |
| Relapsing Polychondritis | Multiple cartilaginous site involvement, systemic symptoms, inflammatory presentation, episodic nature |
| Cellulitis | Erythema and warmth, tenderness, systemic symptoms, acute onset, responds to antibiotics |
Careful clinical evaluation combined with histopathological confirmation distinguishes auricular pseudocyst from these alternative diagnoses and guides appropriate management.
Treatment Modalities
Various therapeutic approaches have been described for managing auricular pseudocysts, ranging from conservative to invasive interventions. Treatment selection depends on lesion characteristics, patient preference, and risk tolerance regarding potential complications.
Conservative Treatment Approaches
Simple Aspiration: The most conservative approach involves needle aspiration of cyst contents using aseptic technique with a 20-gauge needle. While straightforward, simple aspiration alone carries a high recurrence rate, with fluid reaccumulation occurring in a substantial proportion of cases.
Aspiration with Pressure Dressing: Combining aspiration with application of tight, reinforced pressure dressing that encircles the forehead and pinna provides better outcomes than aspiration alone. The pressure dressing is typically maintained for one week, allowing fibrosis and obliteration of the cavity space. This approach significantly reduces recurrence rates compared to aspiration alone.
Corticosteroid Injection: Intralesional injection of corticosteroids following aspiration addresses any inflammatory component and may promote resolution. Systemic oral corticosteroids administered concurrently with aspiration and pressure dressing have demonstrated success in clinical case series. A typical regimen involves starting with prednisolone 40 mg daily and tapering by 10 mg weekly over 3-4 weeks.
Combined Approach
The most effective conservative management combines needle aspiration under aseptic conditions with immediate application of pressure dressing and concurrent systemic corticosteroid therapy. This multimodal approach addresses mechanical evacuation, prevents reaccumulation through pressure application, and reduces inflammatory responses through corticosteroid administration. Clinical experience demonstrates complete resolution without complications or recurrence over extended follow-up periods using this combined protocol.
Invasive Surgical Approaches
Incision and Drainage with Obliteration: More invasive techniques include opening the cyst cavity, complete drainage of contents, and obliteration through curettage combined with sclerosing agent application and pressure dressing.
Open Deroofing: This procedure involves surgical removal of the anterior cartilaginous leaflet of the pseudocyst followed by repositioning of the overlying skin flap. While effective in preventing recurrence, this technique carries significant risks.
Risks of Invasive Approaches: Invasive surgical interventions carry notable complications including perichondritis development, cauliflower ear deformity formation, floppy ear development, and increased recurrence rates despite more extensive intervention. These complications may result in permanent cartilage damage and cosmetic disfigurement.
Treatment Outcomes and Considerations
Conservative approaches utilizing aspiration, pressure dressing, and systemic corticosteroid therapy represent the preferred initial management strategy, providing excellent outcomes with minimal morbidity. The combination approach demonstrates complete resolution rates without complications and minimal recurrence when properly executed. Patients tolerate conservative management well, with minimal downtime and risk of adverse effects compared to surgical intervention.
Surgical intervention should be reserved for cases demonstrating treatment failure with conservative approaches or patient preference for definitive management despite inherent risks. The potential for permanent complications with invasive approaches mandates careful patient counseling regarding risks versus benefits.
Frequently Asked Questions
Q: What exactly is an auricular pseudocyst?
A: An auricular pseudocyst is a benign, asymptomatic cystic swelling of the upper ear containing viscous fluid. It is termed a “pseudocyst” because it lacks an epithelial lining, distinguishing it from true cysts. The condition develops within cartilaginous tissue and typically progresses gradually over weeks.
Q: How common are auricular pseudocysts?
A: Auricular pseudocysts are rare conditions, with limited epidemiological data available. They predominantly affect young adult males, with some studies suggesting higher prevalence in Asian populations. The exact incidence remains undefined due to the relative rarity of reported cases.
Q: What causes auricular pseudocysts to develop?
A: The exact cause remains unknown, though prior traumatic injury to the ear is recognized as a significant initiating factor in many cases. The condition can also develop spontaneously without identifiable trauma. Proposed mechanisms include cartilage fragmentation, inflammatory responses, and congenital cartilage abnormalities.
Q: How is auricular pseudocyst diagnosed?
A: Diagnosis is typically based on clinical history, physical examination revealing characteristic nontender fluctuant swelling, and histopathological analysis confirming intracartilaginous cyst without epithelial lining. The combination of clinical presentation and histology provides definitive diagnosis.
Q: What is the most effective treatment for auricular pseudocyst?
A: Combined conservative management using needle aspiration, pressure dressing application, and systemic corticosteroid therapy demonstrates the highest success rates with minimal complications. This approach provides complete resolution without recurrence in most cases while avoiding risks associated with invasive surgical procedures.
Q: Can auricular pseudocysts recur after treatment?
A: Recurrence rates vary depending on treatment approach. Simple aspiration alone has high recurrence rates, while combined conservative treatment with pressure dressing and corticosteroids significantly reduces recurrence. Even invasive surgical approaches may be followed by recurrence despite more extensive intervention.
Q: What complications can result from auricular pseudocyst treatment?
A: Conservative approaches carry minimal complication risk. Invasive surgical interventions carry greater risks including perichondritis, cauliflower ear deformity, floppy ear development, and permanent cartilage damage. Conservative management is preferred to minimize these potential complications.
Q: Is auricular pseudocyst painful?
A: No, auricular pseudocysts are characteristically nontender and asymptomatic. The absence of pain despite visible swelling is a distinguishing feature that helps differentiate this condition from other ear lesions causing discomfort.
References
- Pseudocyst of the Auricle — Wikipedia. Accessed January 29, 2026. https://en.wikipedia.org/wiki/Pseudocyst_of_the_auricle
- Pseudocyst of the Auricle — Indian Journal of Dermatology, Venereology and Leprology. Published 2008. https://ijdvl.com/pseudocyst-of-the-auricle-2/
- Pseudocyst of the Auricle: A Histologic Perspective — PubMed/NCBI. Published 2004. https://pubmed.ncbi.nlm.nih.gov/15235361/
Similar Articles






Read full bio of Sneha Tete