Benign Lymphoplasmacytic Plaque: Clinical Features and Management
Understanding a rare pediatric skin condition: diagnosis, clinical presentation, and treatment options.

Benign Lymphoplasmacytic Plaque: A Comprehensive Overview
Benign lymphoplasmacytic plaque (LPP) is a rare and distinctive clinicopathological entity that primarily affects children and young individuals. This condition presents as a solitary, asymptomatic, erythematous plaque typically located on the lower extremities, particularly the pretibial or tibial regions. Despite its benign nature, the condition has often been misdiagnosed as an infectious disease or cutaneous lymphoma due to its clinical and histopathological features. Understanding the defining characteristics of this condition is essential for accurate diagnosis and appropriate management.
Clinical Presentation and Characteristics
The clinical presentation of benign lymphoplasmacytic plaque is distinctive and relatively uniform across reported cases. Patients typically present with solitary erythematous to red-brown plaques that are asymptomatic and located primarily on the lower extremities. The lesions are often described as having a linear arrangement or grouped in clusters, with papules converging into larger plaques.
The following clinical features characterize typical presentations:
- Solitary or occasionally clustered lesions on the legs, with the pretibial region being the most common site
- Erythematous to brownish papules and plaques with an irregular surface
- Scaly appearance with focal parakeratosis visible upon examination
- Lesions typically measuring 2-3 centimeters in diameter
- Complete absence of systemic symptoms and constitutional signs
- Chronic course with lesions present for months to years without significant change
- Absence of ulceration, which helps differentiate it from other lymphoproliferative disorders
The condition predominantly affects children and young adults, with documented cases ranging from 3 to 7 years of age. In rare instances, lesions may present in atypical locations such as the wrist, hand, or buttock, though the lower extremities remain the classic presentation site. Unlike many infectious dermatoses, benign lymphoplasmacytic plaque does not respond to standard topical corticosteroids or other conservative treatment modalities.
Histopathological Findings
The diagnosis of benign lymphoplasmacytic plaque is confirmed through histopathological examination of a skin biopsy specimen. The microscopic features are characteristic and reproducible across cases, aiding in differentiation from mimicking conditions.
Key histopathological findings include:
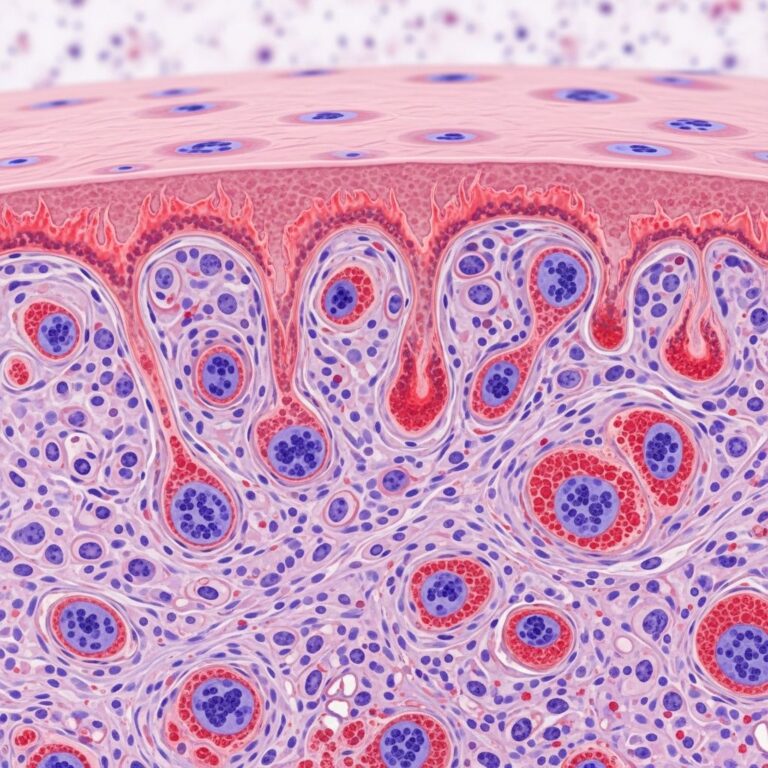
- Focal parakeratosis overlying areas of irregular acanthosis and epidermal hyperplasia
- Dense dermal lymphoid infiltrates admixed with numerous plasma cells extending throughout the dermis
- Perivascular and periadnexal distribution of inflammatory cells, predominantly in the deep dermis
- Occasional epithelioid granulomas without central necrosis
- Extension of plasma cells into the superficial subcutaneous tissue in some cases
- Tingible body macrophages and variable inflammatory background
Immunohistochemical analysis reveals a polyclonal pattern of plasma cells, confirmed by the coexistence of both kappa and lambda light chain-positive cells. This polyclonal nature is crucial for excluding monoclonal lymphoproliferative disorders and cutaneous lymphomas. Mixed inflammation with both B-cell and T-cell lymphocytes is typically observed, indicating a reactive rather than neoplastic process. CD138 immunostaining confirms the prominent plasmacytic nature of the dermal infiltrate.
Microorganisms are not identified on special stains including acid-fast bacilli, Giemsa, and periodic acid-Schiff stains, effectively ruling out infectious etiologies such as tuberculosis, syphilis, or mycobacterial infections.
Diagnostic Criteria and Differential Diagnosis
The diagnosis of benign lymphoplasmacytic plaque is established through clinicopathological correlation, combining characteristic clinical features with specific histopathological findings. A punch or excisional biopsy is necessary to confirm the diagnosis and exclude other conditions in the differential diagnosis.
The differential diagnosis should include the following conditions:
- Primary cutaneous lymphomas: Particularly primary cutaneous marginal zone lymphoma and lymphocytoma cutis, which present with similar clinical features
- Infectious diseases: Secondary syphilis, cutaneous tuberculosis, and other granulomatous infections
- Reactive infiltrates: Jessner lymphocytic infiltration and other benign inflammatory conditions
- Pseudolymphomas: Drug-induced and other benign lymphoid proliferations
- Acanthosis-related conditions: Psoriasiform dermatitis and other reactive epidermal thickening
Serological testing for syphilis and tuberculosis screening via QuantiFERON-TB Gold testing should be performed to exclude infectious etiologies. The polyclonal nature of the plasma cells on immunohistochemistry effectively excludes monoclonal lymphomas, which show clonal populations of plasma cells.
Etiology and Pathogenesis
The exact etiology and pathogenesis of benign lymphoplasmacytic plaque remain unknown. However, current evidence suggests that the condition may result from a local reaction to an unknown, acquired stimulus in a specific age group, particularly in children. The distinctive perivascular and periadnexal distribution of immune cells provides a potential clue toward understanding its pathogenesis.
One intriguing case report has suggested that an insect bite may serve as a causative factor in some instances, though this association requires further investigation and confirmation in additional cases. The chronic nature of the lesions and their resistance to treatment suggest that the inciting stimulus, if present, may persist locally within the dermis. The polyclonal nature of the inflammatory infiltrate indicates a non-malignant, reactive immune response to an unidentified antigen or irritant.
Clinical Course and Prognosis
Benign lymphoplasmacytic plaque is characterized by a chronic and persistent clinical course. Lesions typically remain stable in size and appearance over extended periods, often lasting for years without spontaneous resolution. The condition is entirely benign without potential for transformation or systemic involvement.
Key prognostic features include:
- Excellent overall prognosis with no risk of malignant transformation
- Absence of systemic involvement or constitutional symptoms
- Normal serum lactate dehydrogenase levels, indicating lack of systemic lymphoproliferative disease
- Chronic but stable course without spontaneous regression in most cases
- No documented cases of progression to cutaneous or systemic lymphoma
- Cosmetic concerns may be the primary clinical issue for affected patients
Unlike aggressive cutaneous B-cell lymphomas, benign lymphoplasmacytic plaque does not demonstrate elevated inflammatory markers or systemic manifestations such as fever, night sweats, or weight loss. Laboratory investigations including complete blood count and serum chemistries remain normal.
Treatment and Management Options
The management of benign lymphoplasmacytic plaque is challenging, as the condition demonstrates remarkable resistance to conventional therapeutic approaches. Currently, no universally effective medical treatment exists, making complete surgical excision the only definitively curative option.
Treatment approaches include:
- Topical corticosteroids: Generally ineffective, though some cases show partial remission with potent agents such as 0.3% diflucortolone valerate ointment
- Intralesional steroid injections: May produce partial remission in some patients but do not typically result in complete resolution
- Topical immunomodulators: Tacrolimus hydrate has been attempted with variable and limited success
- Watchful waiting: An acceptable approach for asymptomatic lesions that cause no functional impairment, monitoring for stability or change
- Surgical excision: Complete excision with margins remains the only treatment modality that provides definitive resolution of the lesion
The choice of treatment should be individualized based on patient preference, lesion location, cosmetic concerns, and patient age. For cosmetically concerning lesions or those in functionally important locations, complete surgical excision is recommended. For small, asymptomatic lesions that do not cause cosmetic distress, observation may be appropriate, as the lesions pose no health risk.
Distinguishing Features from Related Conditions
Benign lymphoplasmacytic plaque must be carefully distinguished from several conditions with overlapping clinical and histopathological features. Primary cutaneous marginal zone lymphoma (PCMZL) presents with similar morphological features but demonstrates monoclonal B-cell infiltrates and carries a more significant prognostic implications. Unlike PCMZL, benign lymphoplasmacytic plaque shows polyclonal plasma cell proliferation and lacks potential for systemic involvement.
Lymphocytoma cutis, another benign condition affecting children, presents with reactive germinal centers with normal proliferation rates and various inflammatory cells including eosinophils. However, the pattern and composition of inflammatory infiltrates differ from those in benign lymphoplasmacytic plaque. Additionally, lymphocytoma cutis may be associated with Borrelia infection in some cases, particularly in Europe, whereas such associations have not been consistently documented in benign lymphoplasmacytic plaque.
Special Considerations and Unusual Presentations
While benign lymphoplasmacytic plaque classically presents on the lower extremities, several atypical presentations have been documented in the medical literature. Cases involving the wrist, hand, and buttock have been reported, expanding the potential anatomical distribution of this condition beyond previously recognized patterns. These atypical presentations may increase the risk of misdiagnosis if clinicians anchor primarily on the typical pretibial location.
The clinical presentation of papules converging in a linear plaque or clusters in children should raise suspicion for benign lymphoplasmacytic plaque regardless of anatomical location. Awareness of these atypical presentations is essential for dermatologists and pathologists to prevent delayed diagnosis and unnecessary investigations for infectious diseases or lymphoproliferative disorders.
Frequently Asked Questions
Q: Is benign lymphoplasmacytic plaque contagious?
A: No, benign lymphoplasmacytic plaque is not contagious. It is a localized inflammatory condition with no infectious etiology, though the exact cause remains unknown. Special stains for infectious organisms consistently test negative.
Q: Can benign lymphoplasmacytic plaque transform into a malignant lymphoma?
A: No, there is no documented risk of malignant transformation. The condition is entirely benign with polyclonal, reactive inflammatory infiltrates that do not progress to cutaneous or systemic lymphoma.
Q: What is the expected outcome if the lesion is not treated?
A: Untreated lesions typically remain stable and chronic, persisting for years without spontaneous resolution. While they pose no health risk, they may cause cosmetic concerns. Surgical excision is the only treatment that achieves complete resolution.
Q: Is a biopsy necessary to diagnose benign lymphoplasmacytic plaque?
A: Yes, a punch or excisional biopsy with histopathological examination is necessary to confirm the diagnosis and exclude other conditions such as infectious diseases, reactive infiltrates, and cutaneous lymphomas. Clinicopathological correlation is essential for accurate diagnosis.
Q: Are there any systemic manifestations or complications associated with this condition?
A: No, benign lymphoplasmacytic plaque is an entirely benign condition without systemic involvement or constitutional symptoms. Laboratory markers remain normal, and there is no risk of internal organ involvement or lymph node disease.
References
- B-Cell Lymphomas of the Skin — Plastic Surgery Key. 2024. https://plasticsurgerykey.com/b-cell-lymphomas-of-the-skin-2/
- Lymphoplasmacytic Plaque in Children — National Center for Biotechnology Information (NCBI) / National Institutes of Health (NIH). 2016. https://pmc.ncbi.nlm.nih.gov/articles/PMC4828401/
- Tibial Lymphoplasmacytic Plaque: A New, Illustrative Case of a Rare Condition — S. Karger AG, Medical and Scientific Publishers. 2017. https://karger.com/drm/article/225/1/27/117529
- Lymphoplasmacytic Plaque in Children: Case Report and Literature Review — Université catholique de Louvain (UCLouvain) Open Repository. 2015. https://dial.uclouvain.be/downloader/downloader.php
- Lymphoplasmocytic Plaque in Children: A Report of an Atypical Location — John Wiley & Sons, Inc. / Pediatric Dermatology Journal. 2023. https://onlinelibrary.wiley.com/doi/10.1111/pde.15555
- Jessner Lymphocytic Infiltration of the Skin — National Center for Biotechnology Information (NCBI) / National Institutes of Health (NIH) StatPearls. 2024. https://www.ncbi.nlm.nih.gov/books/NBK562281/
Similar Articles






Read full bio of medha deb