Brunsting-Perry Cicatricial Pemphigoid Pathology
Exploring the pathology of Brunsting-Perry cicatricial pemphigoid: a rare localized variant with scarring bullae on head and neck.

Authors: Dr Achala Liyanage, Dermatology Fellow, Waikato Hospital, Hamilton, New Zealand; Assoc Prof Patrick Emanuel, Dermatopathologist, Auckland, New Zealand. Reviewed January 2015; Updated 2025.
Introduction
Brunsting-Perry cicatricial pemphigoid represents a rare and distinctive variant of cicatricial pemphigoid, primarily manifesting as localized subepidermal blisters predominantly on the head and neck regions. Unlike the classic form of cicatricial pemphigoid, which frequently involves mucous membranes such as the oral cavity, conjunctiva, and genitalia, Brunsting-Perry type is characteristically confined to the skin without mucosal involvement. This condition was first described by Brunsting and Perry in 1957, highlighting its chronic, progressive nature leading to significant scarring and potential complications like scarring alopecia on the scalp.
Clinically, patients present with tense vesicles and bullae that rupture to form erosions, crusts, and atrophic scars, often on the scalp, forehead, face, and neck. The scarring is a hallmark feature, distinguishing it from non-scarring bullous disorders. The disease shows a predilection for older adults, typically those over 60 years, with no strong gender bias reported. Pathogenesis involves autoantibodies targeting components of the dermal-epidermal junction, particularly BP180 (bullous pemphigoid antigen 2), BP230, and laminin 332, leading to subepidermal cleavage.
The localized presentation poses diagnostic challenges, as it mimics other bullous diseases. Accurate histopathological and immunopathological correlation is essential for diagnosis, guiding immunosuppressive therapy to halt progression and minimize scarring. Early recognition prevents irreversible damage, such as blindness from corneal involvement in atypical extensions or permanent hair loss.
Histology
Microscopic examination of lesional skin in Brunsting-Perry cicatricial pemphigoid reveals characteristic subepidermal blistering. The blister forms within the dermal-epidermal junction, specifically below the lamina lucida, creating a clean split with preserved epidermal roof and dermal floor. This subepidermal cleavage is filled with minimal acellular debris in early lesions, progressing to fibrin, erythrocytes, and inflammatory cells in older blisters.
The inflammatory infiltrate varies by lesion stage and chronicity. Early active lesions display a paucicellular blister with sparse neutrophils or eosinophils adjacent to the blister base. Papillary dermal microabscesses, comprising neutrophils or mixed eosinophils, may be evident, resembling bullous pemphigoid. As lesions mature, the infiltrate becomes mixed, including lymphocytes, plasma cells, and histiocytes in the superficial dermis. Chronic lesions show fibrosis and scarring, with thickened collagen bundles, vascular ectasia, and reduced adnexal structures, explaining the cicatricial alopecia observed clinically.
- Early lesions: Subtle subepidermal separation, papillary microabscesses (neutrophilic or eosinophilic).
- Active bullae: Large subepidermal blister, moderate mixed inflammatory infiltrate (lymphocytes, eosinophils, neutrophils).
- Healing/scarred areas: Dermal fibrosis, loss of rete ridges, sparse perivascular lymphoplasmacytic infiltrate.
High-power views highlight dermal-epidermal separation with intact basal keratinocytes on the blister roof. Solar elastosis, reflecting chronic UV exposure, often accompanies scalp lesions due to the photodamaged sites affected. These features underscore the need for sampling perilesional skin to capture diagnostic inflammatory changes.
Special Studies
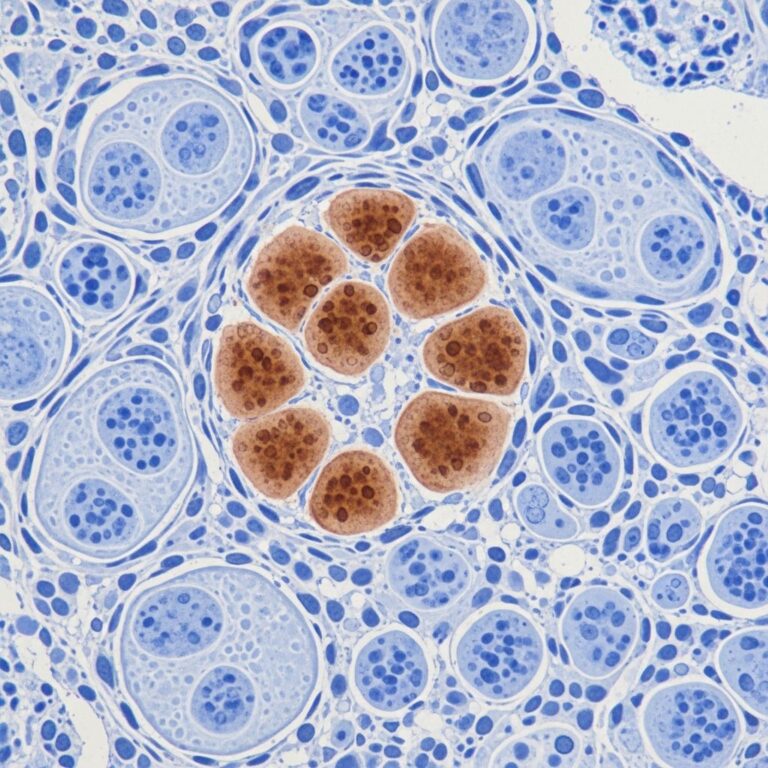
Direct Immunofluorescence (DIF) is pivotal for confirming the diagnosis. DIF of peribullous or perilesional skin demonstrates linear deposition of IgG and/or C3 along the basement membrane zone (BMZ). IgG is most common, often with C3, while IgA or IgM is rare. Salt-split skin immunofluorescence differentiates levels: in Brunsting-Perry, antibodies bind the dermal side, akin to epidermolysis bullosa acquisita (EBA), contrasting with roof-side binding in bullous pemphigoid.
Electron Microscopy (EM) provides ultrastructural precision. The split occurs in the sublamina densa zone, with the blister roof retaining lamina densa and anchoring fibrils. Immune deposits appear granular, attached to and below the lamina densa, mirroring EBA patterns. This supports theories positing Brunsting-Perry as a localized EBA variant.
| Technique | Findings in Brunsting-Perry | Differential Comparison |
|---|---|---|
| Direct IF (routine) | Linear IgG ± C3 at BMZ | Similar to BP, CP; EBA also dermal |
| Salt-split IF | Dermal side binding | BP: epidermal; EBA: dermal |
| Immuno-EM | Deposits below lamina densa | Identical to EBA |
Indirect immunofluorescence and ELISA for anti-BP180/230 or anti-laminin 332 antibodies further characterize autoantibody profiles, aiding therapy selection.
Differential Diagnosis
Brunsting-Perry cicatricial pemphigoid must be differentiated from other subepidermal bullous diseases, particularly those affecting the head and neck.
Localised Bullous Pemphigoid
The primary clinical mimic, localised bullous pemphigoid presents with tense bullae on head/neck without scarring. Histology shows eosinophil-rich infiltrate and papillary microabscesses. DIF reveals epidermal-side IgG on salt-split skin, targeting BP180/230 NC16A domain.
Epidermolysis Bullosa Acquisita (EBA)
Shares dermal BMZ binding and sublamina densa splits. EBA often involves trauma-prone sites with milia/mechano-bullous features; mucosal involvement more common. Brunsting-Perry is distinguished by exclusive head/neck localization and scarring without widespread distribution.
Cicatricial Pemphigoid (Mucous Membrane Pemphigoid)
Classic CP predominantly affects mucosa with variable skin involvement. Brunsting-Perry lacks mucosal disease and is purely cutaneous.
Other Considerations
- Linear IgA Disease: IgA linear BMZ; neutrophilic infiltrate.
- Discoid Lupus Erythematosus: Interface dermatitis, scarring alopecia without blisters.
- Lichen Planus Pemphigoides: Interface changes with subepidermal blisters.
Salt-split DIF and clinical correlation resolve most ambiguities.
Frequently Asked Questions (FAQs)
What is Brunsting-Perry cicatricial pemphigoid?
A rare localized variant of cicatricial pemphigoid causing scarring blisters on head and neck without mucosal involvement.
How is it diagnosed pathologically?
Subepidermal blisters histologically; linear IgG/C3 on DIF with dermal binding on salt-split skin.
Does it scar like classic pemphigoid?
Yes, prominent scarring distinguishes it from non-cicatricial bullous pemphigoid.
Is it related to epidermolysis bullosa acquisita?
Immunopathological overlap suggests Brunsting-Perry may be a localized EBA variant.
What is the treatment?
Topical/systemic corticosteroids, immunosuppressants like hydroxychloroquine, dapsone; severe cases require rituximab or cyclophosphamide.
Clinical Implications and Management
Given its scarring propensity, prompt diagnosis via biopsy and DIF is crucial. Therapy aims to suppress autoantibody production and inflammation. First-line includes superpotent topical steroids (clobetasol) with or without tacrolimus for limited disease. Systemic agents like prednisone, dapsone, or hydroxychloroquine follow; rituximab for refractory cases. Monitoring prevents complications like squamous cell carcinoma in chronic scars. Multidisciplinary care involving dermatology, ophthalmology (if extension), and pathology optimizes outcomes.
Recent cases highlight scalp exclusivity with trichodynia and alopecia, emphasizing trichoscopy’s role: bullae, erosions, comma vessels, scar plaques. Photodamage often coexists, suggesting UV triggers.
References
- Brunsting-Perry cicatricial bullous pemphigoid: a clinical variant of localized acquired epidermolysis bullosa? — P Joly et al. Journal of the American Academy of Dermatology. 1993-01-01. https://pubmed.ncbi.nlm.nih.gov/8425977/
- Brunsting-Perry cicatricial pemphigoid pathology — DermNet NZ. 2015-01-01 (reviewed). https://dermnetnz.org/topics/brunsting-perry-cicatricial-pemphigoid-pathology
- Brunsting-Perry Cicatricial Pemphigoid of the Scalp — JCS Guerrero. International Journal of Clinical Medical Case Reports. 2025. https://ijclinmedcasereports.com/pdf/IJCMCR-LE-01210.pdf
- Cicatricial Pemphigoid of Brunsting-Perry — B Michel et al. Archives of Dermatology. 1977. https://jamanetwork.com/journals/jamadermatology/fullarticle/537809
- Secondary Cicatricial Scalp Alopecia Caused by Brunsting-Perry Pemphigoid — Cureus. 2024. https://www.cureus.com/articles/306599-secondary-cicatricial-scalp-alopecia-caused-by-brunsting-perry-pemphigoid-a-case-report
Similar Articles






Read full bio of medha deb