Cholesterol Emboli: Causes, Signs, Treatments, And Prevention
Understanding cholesterol emboli syndrome: causes, skin signs, diagnosis, and management of this rare vascular condition.

What is cholesterol emboli?
Cholesterol emboli, also known as atheroembolic disease or cholesterol crystal embolization, is a rare but serious condition where small fragments of cholesterol-rich atherosclerotic plaque break off from larger arteries, particularly the aorta, and travel through the bloodstream to lodge in smaller distal arteries. These emboli, often needle-shaped cholesterol crystals, obstruct blood flow, trigger inflammation, and cause ischaemic damage to downstream tissues and organs.
This syndrome typically affects elderly patients with advanced atherosclerosis. It differs from thromboembolism, where larger clots cause acute blockages; cholesterol emboli lead to a subacute or chronic process with progressive multi-organ dysfunction.
Commonly implicated sites for plaque disruption include the abdominal aorta, iliac arteries, and branches of the femoral arteries. Emboli most frequently impact the lower extremities, kidneys, skin, gastrointestinal tract, pancreas, and central nervous system.
Who gets cholesterol emboli?
Cholesterol emboli predominantly affect older adults over 60 years, with a male predominance. Risk factors mirror those for atherosclerosis:
- Advanced age
- Hypertension
- Hyperlipidaemia (high cholesterol)
- Diabetes mellitus
- Tobacco smoking
- Coronary artery disease
- Peripheral vascular disease
- Abdominal aortic aneurysm
- Previous stroke or transient ischaemic attack
The condition is often precipitated by invasive vascular procedures that manipulate or destabilize plaques, occurring in up to 3% of cases post-catheterization.
What causes cholesterol emboli?
Atherosclerotic plaques in large arteries develop a fibrous cap over a lipid-rich core containing cholesterol crystals. Disruption of this cap releases showers of crystals into the circulation. Triggers include:
- Vascular interventions: Aortic or cardiac catheterization (most common, e.g., coronary angiography, angioplasty), vascular surgery (endarterectomy, aneurysm repair), fibrinolytic therapy.
- Spontaneous: Anticoagulation (warfarin), hypertension surges, trauma, or unprovoked plaque rupture in unstable plaques.
Once embolized, crystals lodge in arterioles <150 μm in diameter, causing mechanical occlusion, endothelial damage, and a local inflammatory response with complement activation and eosinophil recruitment.
What are the signs and symptoms of cholesterol emboli?
Clinical presentation is variable, often subacute over days to weeks, with constitutional symptoms preceding organ-specific manifestations. Systemic signs include fever, fatigue, weight loss, myalgias, and anorexia due to inflammatory response.
Skin findings
Dermatological signs are classic and occur in ~30-80% of cases, aiding early recognition:
- Blue toe syndrome: Painful cyanotic toes or livedo reticularis (mottled, net-like purplish discoloration on feet/legs).
- Subungual splinter haemorrhages
- Tender purpuric nodules or ulcers on distal extremities
- Digital gangrene
- Angiokeratomas (small red-purple papules)
Skin involvement reflects distal embolization to dermal arterioles.
Renal involvement
Kidneys are affected in 30-80% (most common organ), causing acute kidney injury (AKI) or rapidly progressive renal failure. Urine shows haematuria, proteinuria, eosinophiluria; eosinophilia in 80%.
Gastrointestinal
13-18%: Abdominal pain, bleeding, diarrhoea, pancreatitis, bowel ischaemia/infarction.
Neurological
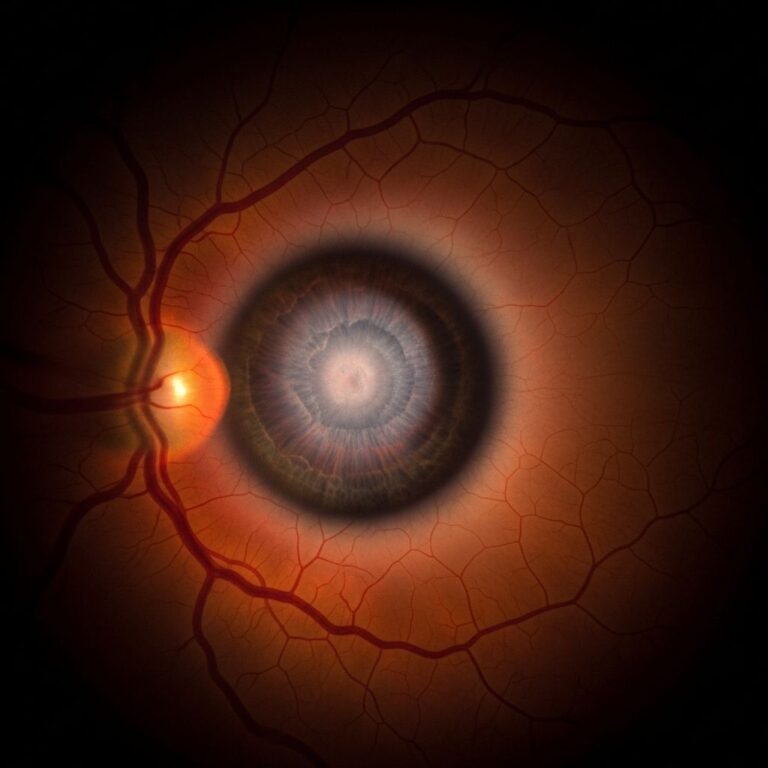
Stroke, confusion, visual loss (retinal artery occlusion), spinal cord ischaemia.
Other
- Musculoskeletal: Limb pain, rhabdomyolysis
- Cardiac: Myocardial infarction, valve dysfunction
- Systemic: Eosinophilia, elevated ESR/CRP, hypocomplementaemia
| Organ/System | Frequency | Key Manifestations |
|---|---|---|
| Kidneys | 31-80% | AKI, proteinuria, eosinophiluria |
| Skin | 15-50% | Blue toes, livedo reticularis, gangrene |
| GI Tract | 13-20% | Pain, bleeding, pancreatitis |
| Brain/CNS | 10-30% | Stroke, visual loss |
| Muscles | ~10% | Pain, elevated CK |
How is cholesterol emboli diagnosed?
Diagnosis combines clinical suspicion (post-procedure multi-organ dysfunction in atherosclerotic patient), lab findings (eosinophilia >5%, elevated creatinine), and histopathology.
- Biopsy: Gold standard – skin, muscle, kidney, or gut biopsy showing biconvex cholesterol clefts in arterioles (pathognomonic).
- Fundoscopy: Hollenhorst plaques (retinal cholesterol emboli).
- Labs: Anaemia, thrombocytopenia, high ESR/CRP, urinary eosinophils.
- Imaging: Doppler ultrasound, CT/MR angiography (rarely diagnostic).
Differential includes vasculitis, endocarditis, DIC, cryoglobulinaemia.
What is the treatment for cholesterol emboli?
No specific therapy; management is supportive and preventative:
- Avoid triggers: Minimize invasive procedures; use embolic protection devices.
- Symptomatic: Statins for plaque stabilization, blood pressure control, dialysis for renal failure.
- Anti-inflammatories: Steroids/IL-6 inhibitors (limited evidence).
- Anticoagulation caution: May worsen embolization.
What is the outcome for cholesterol emboli?
Prognosis poor: 30-90% mortality at 2 years, mainly from renal failure/cardiac events. Early recognition improves survival; recurrent embolization worsens outlook.
How can cholesterol emboli be prevented?
- Risk factor modification: Smoking cessation, statins, antihypertensives, diabetes control.
- Periprocedural: Gentle catheter manipulation, distal embolic filters, pre-op statins.
- Avoid systemic anticoagulation in high-risk patients without clear indication.
Related topics
- Atherosclerosis
- Blue toe syndrome
- Livedo reticularis
- Acute kidney injury
- Antiphospholipid syndrome
Frequently Asked Questions
Q: What triggers cholesterol emboli after catheterization?
A: Plaque disruption from catheter manipulation releases cholesterol crystals into circulation, lodging in distal arteries.
Q: Is blue toe always cholesterol emboli?
A: No, differentials include embolism, vasculitis, or cryoglobulinaemia; biopsy confirms.
Q: Can cholesterol emboli be treated with surgery?
A: Surgery risks further embolization; conservative management preferred unless critical limb ischaemia.
Q: Does statin therapy help after diagnosis?
A: Yes, statins stabilize plaques and reduce inflammation, improving outcomes.
References
- Cholesterol Embolism: Causes, Symptoms, and Treatments — Healthline. 2023. https://www.healthline.com/health/high-cholesterol/cholesterol-embolism
- Cholesterol Emboli — MD Searchlight. 2024-01-15. https://mdsearchlight.com/heart-health/cholesterol-emboli/
- Cholesterol Emboli: Symptoms, Causes & Treatment — Cleveland Clinic. 2024-03-20. https://my.clevelandclinic.org/health/diseases/24575-cholesterol-emboli
- What is a cholesterol embolism? — Medical News Today. 2023-11-10. https://www.medicalnewstoday.com/articles/what-is-a-chloesterol-embolism
- Cholesterol Embolization Syndrome — Stroke Manual. 2024. https://www.stroke-manual.com/cholesterol-embolization-syndrome/
- Cholesterol Emboli Syndrome (When Artery Plaques …) — YouTube (Educational Video). 2023. https://www.youtube.com/watch?v=rvE02GktR-8
Similar Articles






Read full bio of Sneha Tete