Coccidioidomycosis Pathology: Clinical And Histologic Guide
Detailed histopathology and clinical insights into coccidioidomycosis, the Valley fever fungal infection.

Author: Dr. Harriet Cheng, Dermatopathologist / Dermatologist, Hamilton, New Zealand.
Introduction
Coccidioidomycosis, commonly known as Valley fever, is a systemic mycosis caused by the dimorphic fungi Coccidioides immitis and C. posadasii. These pathogens are endemic to arid regions of the southwestern United States, northern Mexico, and parts of Central and South America. Infection occurs primarily through inhalation of airborne arthroconidia from soil disturbed by wind or human activity. While approximately 60% of infections are asymptomatic, symptomatic cases range from self-limited pneumonia to severe disseminated disease, particularly in immunocompromised individuals, pregnant women, and those of African or Filipino descent.
The pathology is characterized by the unique transformation of the fungus from mycelial form in the environment to large spherules in host tissues, eliciting acute and chronic inflammatory responses. This article details the histopathological features, clinical manifestations, and diagnostic considerations, drawing from tissue reactions observed in skin, lung, and disseminated sites.
Histology of Coccidioidomycosis
Histopathological examination reveals distinctive fungal elements amid varied inflammatory patterns. The hallmark is the presence of spherules, which are round to oval structures measuring 20–150 μm in diameter, filled with endospores of 2–5 μm. Immature spherules appear empty, while mature ones contain numerous endospores. Ruptured spherules release endospores, triggering intense neutrophilic and eosinophilic infiltration.
Tissue responses include:
- Suppurative granulomatous inflammation: Central suppuration with neutrophils, surrounded by granulomas featuring epithelioid histiocytes, multinucleated giant cells, and lymphocytes.
- Eosinophilic abscesses: Prominent eosinophils, especially in early lesions or disseminated disease.
- Non-necrotizing granulomas: In chronic or contained infections, with spherules engulfed by macrophages.
- Pseudohyphae or aberrantly shaped forms: Rare, artifactual appearances mimicking other fungi.
In skin biopsies, lesions show dermal abscesses with spherules, often in verrucous plaques or ulcers. Pulmonary pathology features bronchopneumonia with spherules in alveolar spaces, progressing to cavitation or miliary patterns in dissemination.
Cytology of Coccidioidomycosis
Cytological specimens from bronchoalveolar lavage, fine-needle aspirates, or skin scrapings demonstrate spherules and endospores against a background of acute inflammation. Papanicolaou or Giemsa stains highlight the thick double-contoured walls of spherules. Eosinophils are frequently noted, aiding in rapid presumptive diagnosis. Sensitivity is high in disseminated cases but lower in localized pneumonia.
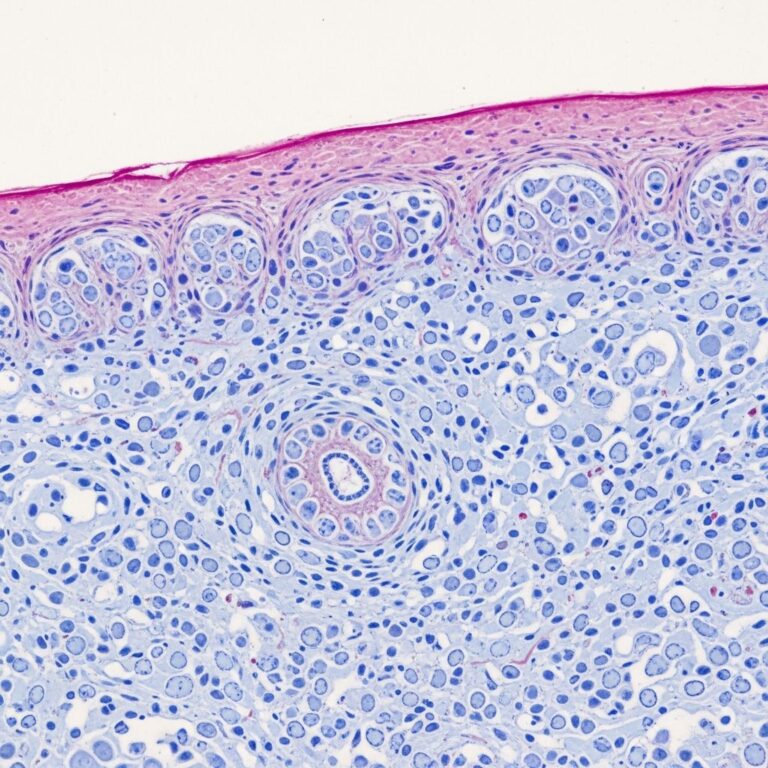
Histopathology Images
Low power view: Dermal suppurative granuloma with central necrosis containing numerous spherules (H&E).
High power: Mature spherule (80 μm) releasing endospores amid neutrophils and eosinophils (PAS).
Polarized light: Empty immature spherule with thick refractile wall (H&E).
These features are pathognomonic, distinguishing coccidioidomycosis from histoplasmosis (smaller yeasts) or blastomycosis (broad-based budding).
Fungal Stains
Special stains enhance visibility:
- Grocott methenamine silver (GMS): Blackens spherule walls and endospores against green background.
- Periodic acid-Schiff (PAS): Magenta staining of fungal elements.
- Mucicarmine: Negative, unlike Cryptococcus.
Immunohistochemistry with anti-Coccidioides antibodies is emerging for confirmation in ambiguous cases.
Differential Diagnosis by Pattern
| Pattern | Key Features | Differential |
|---|---|---|
| Suppurative granulomas with spherules | Spherules 30–80 μm with endospores | Pathognomonic for Coccidioides |
| Eosinophilic abscesses | Prominent eosinophils, ruptured spherules | Parasites (e.g., dirofilaria), bacterial abscess |
| Non-specific granulomas | No organisms seen | Mycobacteria, sarcoidosis |
| Verrucous epidermal hyperplasia | Spherules in dermis | Chromoblastomycosis, deep dermatophytes |
Pathogenesis
Inhaled arthroconidia (3–5 μm) evade mucociliary clearance and transform into spherules at body temperature and CO2 levels. Spherules mature, endosporulate, and rupture, releasing 200–300 endospores that disseminate locally or hematogenously. Host defenses involve alveolar macrophages and neutrophils, but cell-mediated immunity (Th1 response) is crucial for control. Virulence factors include SOWgp protein, urease, and melanin, evading phagocytosis.
Dissemination risk factors: High inoculum, T-cell defects (HIV, transplants), pregnancy (3rd trimester), ethnicity (Filipino, African American).
Clinical Features
Primary infection: Flu-like illness (fever, cough, arthralgias) 1–3 weeks post-exposure. Erythema nodosum/multiforme in 20–30%, more in women. Chest X-ray shows infiltrates or nodules.
- Pulmonary forms: Pneumonia, cavities, miliary disease.
- Cutaneous: 15–20% of dissemination; macules, verrucous lesions, ulcers.
- Musculoskeletal: Osteomyelitis (vertebrae), arthritis (knees).
- Meningitis: Basilar, with eosinophils in CSF; fatal if untreated.
Who is at Risk of Complications?
- Immunocompromised: HIV (CD4 <250), organ transplants, TNF inhibitors.
- Diabetes, chronic lung disease.
- Pregnancy, especially 3rd trimester.
- Racial predisposition: Filipinos > Africans > others.
- High occupational exposure (construction, agriculture).
Investigations
- Serology: IgM (acute), IgG (chronic); complement fixation titer correlates with severity.
- Culture: Sabouraud agar; hazardous, BSL-3 required.
- Imaging: CT for cavities, bone lesions.
- Biopsy: Gold standard for pathology.
Frequently Asked Questions
What does coccidioidomycosis look like histologically?
Characteristic large spherules (20–150 μm) with endospores in suppurative granulomas, highlighted by GMS/PAS stains.
Is eosinophilia common in tissue?
Yes, prominent eosinophils accompany ruptured spherules, mimicking parasitic infection.
Can it mimic bacterial abscess?
Absolutely; deep biopsies are needed to reveal spherules.
How to distinguish from histoplasmosis?
Spherules are much larger than 2–4 μm yeasts; no narrow-based budding.
Is skin involvement primary or secondary?
Rarely primary; usually disseminated hematogenous spread.
Related Topics
- Coccidioidomycosis clinical features
- Histopathology index
- Fungal skin infections
References
- Coccidioidomycosis – StatPearls — NCBI Bookshelf, National Institutes of Health. 2023-08-14. https://www.ncbi.nlm.nih.gov/books/NBK448161/
- Coccidioidomycosis: Epidemiology, Fungal Pathogenesis, and Clinical Management — PubMed Central (PMC). 2021-07-16. https://pmc.ncbi.nlm.nih.gov/articles/PMC8340492/
- Coccidioidomycosis Factsheet — Center for Food Security and Public Health, Iowa State University. 2020. https://www.cfsph.iastate.edu/Factsheets/pdfs/coccidioidomycosis.pdf
- Clinical Overview of Valley Fever (Coccidioidomycosis) — Centers for Disease Control and Prevention (CDC). 2024-05-10. https://www.cdc.gov/valley-fever/hcp/clinical-overview/index.html
- Review of Clinical and Laboratory Diagnostics for Coccidioidomycosis — Journal of Clinical Microbiology, ASM. 2023-01-18. https://journals.asm.org/doi/10.1128/jcm.01581-22
Similar Articles






Read full bio of medha deb