Dermoscopy Of Seborrhoeic Keratosis: 5 Essential Patterns
Master dermoscopic patterns and diagnostic clues for accurate identification of seborrhoeic keratoses in clinical practice.

Seborrhoeic keratoses (SKs), also known as seborrheic keratoses, are among the most common benign epidermal tumours encountered in dermatological practice. These lesions typically appear in middle-aged and older adults, presenting as waxy, stuck-on plaques that vary in colour from light brown to black. While clinically distinctive, dermoscopy enhances diagnostic accuracy by revealing specific microscopic structures that confirm the diagnosis and help differentiate SKs from malignant mimics such as melanoma. This article explores the clinical presentation, histopathological basis, key dermoscopic features, variants, and diagnostic pitfalls of SKs.
Clinical Features of Seborrhoeic Keratoses
SKs are prevalent in individuals over 50 years, with incidence increasing with age. They favour sun-exposed sites, particularly the back, face, chest, and upper limbs, though they can occur anywhere except mucosal surfaces. Studies indicate a higher prevalence in males and lighter skin types (Fitzpatrick skin types I-II), where lesions tend to be smaller (<6 mm) or larger (>6 mm) and lightly pigmented.
Clinically, SKs manifest as round to oval, elevated plaques with a verrucous or stuck-on appearance. Colours range from flesh-toned to dark brown or black, influenced by skin type: lighter shades dominate in fair skin, while bluish hues appear across darker types except ST I. Surfaces often feature hyperkeratosis, giving a warty texture, and sizes vary from millimetres to several centimetres. Multiple lesions are common, but solitary SKs warrant caution for malignancy.
- Common locations: Trunk (especially back), face, extremities.
- Demographics: More frequent in males; peaks in 36-96 age range.
- Skin type variations: Lightly pigmented in ST I-II; darker or bluish in ST III-VI.
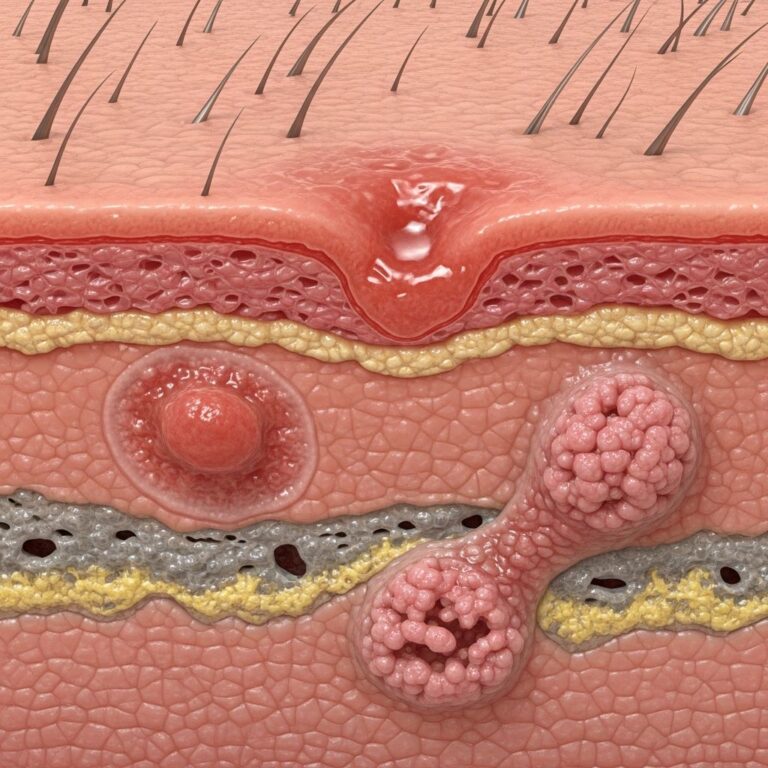
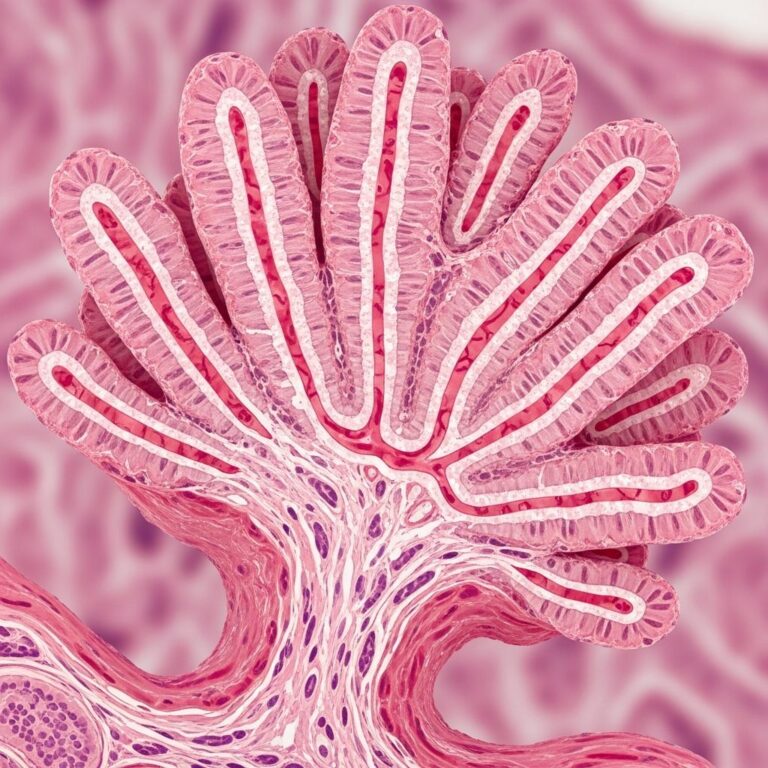
Histopathology of Seborrhoeic Keratoses
Histologically, SKs arise from epidermal hyperplasia of basaloid keratinocytes, exhibiting papillomatous architecture with hyperkeratosis and acanthosis. Key features include horn cysts (true keratin-filled pseudocysts) and pseudo-horn cysts (horny invaginations). The acanthotic type, the most common, shows pronounced basaloid cell proliferation with moderate papillomatosis. Melanocytic hyperplasia may occur in one-third of cases, contributing to pigmentation.
Other variants include hyperkeratotic (thickened stratum corneum), irritated (inflamed with squamous eddies), and melanoacanthoma (prominent melanocytes). These correlate directly with dermoscopic findings, where keratin-filled structures appear as cysts or openings.
Main Dermoscopic Patterns
Dermoscopy of SKs reveals a network of gyri and sulci (cerebriform pattern), comedo-like openings, and milia-like cysts as hallmark features. These patterns vary by subtype but collectively enable high diagnostic confidence.
Acanthotic Seborrhoeic Keratosis
The most frequent subtype displays a thickened epidermis with scattered white clods (milia-like cysts) and grainy brown-black plugs (comedo-like openings). A cerebriform pattern of ridges and fissures predominates, often with sharp borders.
Hyperkeratotic Seborrhoeic Keratosis
Characterized by a thick, white-yellow keratin crust obscuring underlying structures. Dermoscopy may show fissures, ridges, and stuck-on scales. Fat finger-like projections (thick curved ridges) are common.
Irritated or Inflamed Seborrhoeic Keratosis
Features haemorrhagic crusts, glomerular or hairpin vessels, and a white halo. Inflammation reveals dotted or polymorphous vessels amid keratin debris.
Melanotic Seborrhoeic Keratosis
Pigmentation manifests as fingerprint-like ridges, diffuse brown structureless areas, or aggregated globules. Blue-grey ovoid nests may mimic melanoma but lack atypia.
Stucco Keratosis
A variant on lower legs/ankles with milia-like cysts and sharp demarcation, often multiple and small.
Key Dermoscopic Structures
Specific structures underpin SK diagnosis:
- Comedo-like openings: Round/ovoid craters with brown-black keratin plugs, most common feature alongside fat fingers.
- Milia-like cysts: White-yellow roundish clods; cloudy/hazy in SKs vs. starry in nevi/melanoma. More visible in non-polarized mode.
- Fissures and ridges (gyri-sulci): Cerebriform network of white/brown lines.
- Fingerprint-like ridges: Curved thin ridges, especially in pigmented variants.
- Moth-eaten borders: Notched, irregular edges.
- Network-like structures: Interlacing fissures; least common.
- Fat fingers: Thick, finger-like projections; prevalent in lighter skin types.
- Hyperkeratosis/surface scaling: Yellow-white areas.
| Feature | Lighter Skin (ST I-II) | Darker Skin (ST III-VI) |
|---|---|---|
| Fat fingers & looped vessels | Common (p<0.05) | Less common |
| Sharply demarcated borders, fingerprinting, hyperkeratosis | Less | More frequent |
| Comedo openings | Most common overall | Common |
Vascular Patterns in Seborrhoeic Keratoses
Vessels in SKs are typically hairpin, comma, or dotted, surrounded by white keratin. Looped vessels favour lighter skin types. Atypical vascular patterns (e.g., polymorphous in irritated SKs) must be contextualized.
Dermoscopy of Pigmented Seborrhoeic Keratoses
Pigmented SKs show structureless brown areas, fingerprint ridges, or clods. Variation by skin type: light in ST I-II, darker/bluish in others. Avoid mistaking blue-grey nests for melanoma regression.
Diagnostic Clues and Pitfalls
SKs are reliably diagnosed dermoscopically, but pitfalls include SK-like melanomas (82% detected by dermoscopy). Red flags: pigment network, blue-white veil, irregular globules/dots, streaks/pseudopods, blue-black sign (most predictive, OR significant).
- Benign clues: Milia-like cysts, comedo openings, sharp borders, uniform keratin.
- Malignant mimics: Atypical network (periphery), blue-white veil, regression structures.
- Use immersion fluid for hyperkeratotic lesions; polarized light may obscure cysts.
Solitary/irritated SKs or those in low-SK patients heighten suspicion.
Frequently Asked Questions (FAQs)
Q: What are the most common dermoscopic features of seborrhoeic keratoses?
A: Comedo-like openings, milia-like cysts, fat fingers, fissures/gyri-sulci, and hairpin vessels.
Q: How do SKs differ dermoscopically in skin types?
A: Lighter skin shows more fat fingers/looped vessels; darker skin has sharper borders and fingerprinting.
Q: Can melanoma mimic seborrhoeic keratosis?
A: Yes, but dermoscopy reveals pigment network, blue-white veil, or blue-black sign in 82% of cases.
Q: When should a suspected SK be biopsied?
A: If solitary, rapidly growing, symptomatic, or showing atypical dermoscopic features like irregular network or streaks.
Q: Are milia-like cysts visible in polarized dermoscopy?
A: Often less conspicuous; non-polarized mode enhances visibility.
References
- Clinical and Dermatoscopic Features of Seborrheic Keratoses — Omondi et al. 2023-10-01. https://pmc.ncbi.nlm.nih.gov/articles/PMC10656179/
- Seborrheic Keratosis – StatPearls — Sharma S, et al. 2023-08-08. https://www.ncbi.nlm.nih.gov/books/NBK545285/
- Dermoscopic Clues for Diagnosing Melanomas That Resemble Seborrheic Keratoses — Lallas A, et al. 2017-11-01. https://jamanetwork.com/journals/jamadermatology/fullarticle/2612723
- Seborrheic keratoses – dermoscopedia — Dermoscopedia.org. 2023. https://dermoscopedia.org/Seborrheic_keratoses
- Clinical and Dermatoscopic Features of Seborrheic Keratoses — Omondi et al. 2024. https://dpcj.org/index.php/dpc/article/view/2624
- Seborrhoeic keratosis – Primary Care Dermatology Society — PCDS. 2023. https://www.pcds.org.uk/clinical-guidance/seborrhoeic-keratosis-syn-seborrhoeic-wart-basal-cell-papilloma
Similar Articles






Read full bio of medha deb