Dilated Pore of Winer: Pathology and Clinical Characteristics
Understanding the pathological features and clinical presentation of dilated pores of Winer in dermatology.

Dilated Pore of Winer: Understanding the Pathology
A dilated pore of Winer is a benign adnexal tumor with follicular differentiation that presents as a solitary, enlarged comedo typically found on the face and upper trunk of adults. First described by dermatologist Louis H. Winer in 1954, this condition has become recognized as a distinct clinical and histopathological entity rather than a simple variant of other skin lesions. The condition is characterized by a prominent, open comedone appearance with a distinctive black or dark-colored central plug composed of keratin and oxidized sebaceous material.
Clinical Presentation and Morphology
Dilated pores of Winer present with distinctive clinical features that aid in diagnosis. The lesion typically appears as a solitary, enlarged pore with a dark plug in the center, resembling an exaggerated blackhead. The characteristic appearance includes:
- A single, prominent enlarged pore measuring 1-2 millimeters to over 1 centimeter in diameter
- A black or dark-brown central plug composed of keratin and oxidized sebaceous material
- A well-defined margin with normal, healthy-appearing surrounding skin
- A distinctly open central pore or ostium visible on examination
- Non-palpable characteristics due to lack of infiltration into deeper tissue
The lesion is typically non-tender and does not cause physical symptoms unless subjected to chronic manipulation, squeezing, or expression, which may lead to inflammation, infection, or discharge of the keratinous material. Patients may report observing black powdery material discharge, particularly after morning pressure or manipulation.
Anatomical Location
While dilated pores of Winer most commonly occur on the face and head, particularly on the nose and cheeks, they can also develop on other areas. The trunk, especially the back, represents a secondary common location. The preference for these sun-exposed and sebaceous-rich areas suggests a potential role of solar damage and follicular abnormalities in the pathogenesis of these lesions.
Histopathological Features
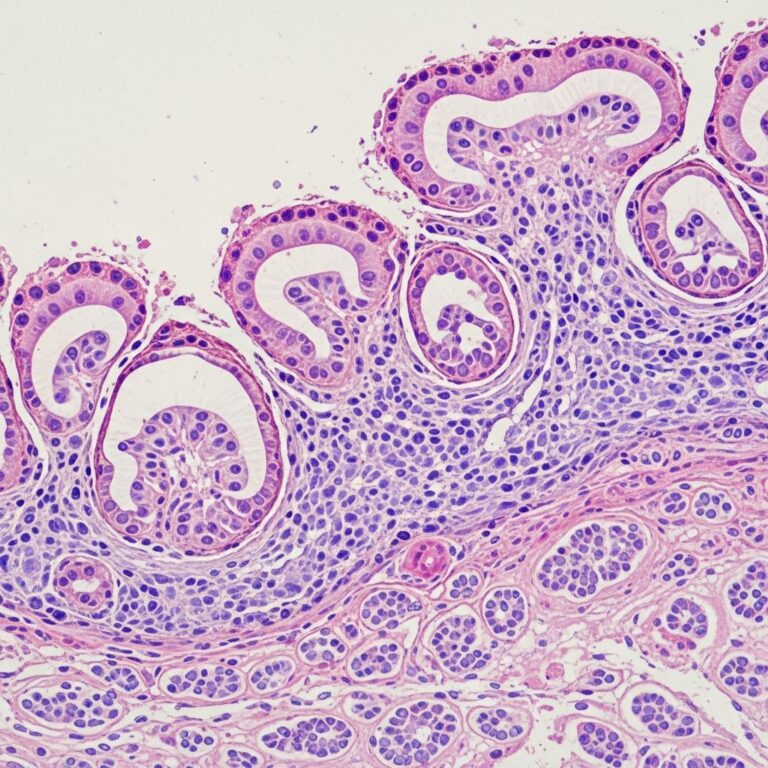
The histological examination of dilated pore of Winer reveals characteristic microscopic features that distinguish it from other skin lesions. The defining pathological findings include:
- A markedly dilated infundibulum (the portion of the hair follicle extending from the sebaceous duct to the surface epidermis)
- Atrophic or thin epithelial lining near the ostium (surface opening), which gradually becomes acanthotic and hypertrophic in deeper portions
- The cystic cavity filled with basket-weave pattern cornified debris that simulates normal stratum corneum, often with increased thickness
- Atrophic hair structures beneath the dilated infundibulum, representing rudimentary or degenerated follicular components
- A flask-shaped or cup-like appearance of the cystic structure extending into the dermis
These histological features confirm that dilated pore of Winer represents a true follicular tumor with differentiation toward hair structures, rather than simply a giant comedone. The pathology reflects an abnormal follicular development with pronounced dilation of the follicular infundibulum and retention of keratinous material.
Distinguishing from Similar Conditions
Clinical and histopathological differentiation from other skin lesions is essential for accurate diagnosis. Dilated pore of Winer must be distinguished from several conditions:
Dilated Pore of Winer vs. Blackheads
The primary difference between a dilated pore of Winer and a typical blackhead is size and depth. A blackhead is a comedo with oxidized sebaceous and keratinous material in a regular follicle, while a dilated pore of Winer represents a markedly enlarged follicular structure with significantly greater keratin accumulation. Blackheads typically measure only a few millimeters, whereas dilated pores of Winer range from several millimeters to over 1 centimeter.
Dilated Pore of Winer vs. Comedo Nevus
Comedo nevus and dilated pore of Winer are distinct entities despite similar appearances. Comedo nevus typically presents as multiple lesions (not solitary), appears in childhood or adolescence (not adulthood), often demonstrates a linear or grouped distribution, and is frequently located on unilateral sites with involvement of face, trunk, and upper arms. Histologically, comedo nevus shows epidermal invaginations with keratin plugs rather than the markedly dilated infundibulum characteristic of dilated pore of Winer.
Dilated Pore of Winer vs. Malignant Lesions
Although dilated pore of Winer is benign, it can occasionally resemble basal cell carcinoma or other malignant lesions, particularly if inflamed or infected. Clinical evaluation by a dermatologist is essential to exclude malignant transformation, though this is exceedingly rare.
Epidemiology and Risk Factors
Dilated pores of Winer demonstrate distinct demographic patterns. These lesions occur predominantly in adults, typically appearing after the age of 40, with increased frequency in older populations. Males are significantly more likely to develop these lesions compared to females. The condition appears more common in individuals of European descent.
The exact etiopathogenesis remains incompletely understood, though several factors have been associated with development. Some studies suggest a correlation with a history of severe or cystic acne, chronic sun exposure, and follicular pathology. The follicular-based origin of these lesions suggests abnormal follicular development with progressive keratin accumulation and follicular dilation.
Formation Mechanism
Dilated pore of Winer forms through a process similar to comedone formation but with progressive enlargement of the follicular structure. The formation process involves:
- Clogging of the hair follicle with dead skin cells and sebaceous material
- Accumulation of keratin and sebum within the follicle, creating increased pressure
- Progressive dilation of the follicular infundibulum as material continues to accumulate
- Oxidation of the accumulated material when exposed to air, creating the characteristic black or dark appearance
- Potential chronic irritation from manipulation or environmental exposure, leading to further follicular enlargement
Clinical Diagnosis
While clinical examination often suggests the diagnosis based on characteristic morphology, histopathological examination provides definitive diagnosis. Excision biopsy is the primary diagnostic procedure, which simultaneously serves as a therapeutic intervention. The biopsy specimen should be examined for the characteristic markedly dilated infundibulum, atrophic epithelium near the ostium, and acanthotic epithelium deeper within the lesion, along with subinfundibular atrophy of hair structures.
Recurrence and Complications
Incomplete removal of dilated pore of Winer may result in recurrence at the same site. Cases treated with incomplete curettage or surface removal without deep and wide excision have demonstrated recurrence after several months. Chronic manipulation or squeezing may lead to secondary inflammation and infection of surrounding tissue, necessitating proper surgical management to prevent such complications.
Treatment Considerations
While the pathological understanding of dilated pore of Winer has advanced significantly, treatment approaches remain primarily surgical. The histopathological features guide surgical planning, as the entire dilated infundibulum and surrounding tissue must be removed to prevent recurrence. Complete excision with adequate margins ensures removal of the entire abnormal follicular structure.
Frequently Asked Questions (FAQs)
Q: Is a dilated pore of Winer cancerous?
A: No, dilated pore of Winer is a benign tumor that is not cancerous. However, dermatological evaluation is important to exclude other potentially harmful lesions with similar appearance.
Q: Why is it called a dilated pore of Winer?
A: The condition was first described and characterized by dermatologist Louis H. Winer in 1954, and the lesion was named after him to recognize his contribution to dermatological literature.
Q: What is the primary difference between a blackhead and a dilated pore of Winer?
A: The primary difference is size and follicular structure. A dilated pore of Winer is much larger than a blackhead and represents a markedly dilated follicular infundibulum rather than a simple comedone.
Q: Can dilated pore of Winer be treated without surgery?
A: No medical (non-surgical) treatment is available for dilated pore of Winer. Surgical excision with complete removal of the dilated infundibulum is the standard treatment approach.
Q: What happens if a dilated pore of Winer is not completely removed?
A: Incomplete removal may result in recurrence of the lesion at the same site. Complete deep and wide excision is necessary to prevent recurrence.
Q: Who is most likely to develop a dilated pore of Winer?
A: Older adult males, particularly those over 40 years of age and of European descent, are most likely to develop dilated pores of Winer.
References
- Dilated pore of Winer — Indian Journal of Dermatology, Venereology, and Leprology (IJDVL). 2013. https://ijdvl.com/dilated-pore-of-winer/
- Dilated Pore of Winer: What Is It, Causes, Symptoms & Treatment — Cleveland Clinic. 2024. https://my.clevelandclinic.org/health/diseases/21796-dilated-pore-of-winer
Similar Articles






Read full bio of Sneha Tete