Disseminate and Recurrent Infundibulofolliculitis
Rare pruritic follicular eruption common in dark-skinned individuals, affecting trunk and extremities with variable treatment responses.

Disseminate and recurrent infundibulofolliculitis (DRIF) is a rare dermatological condition characterized by recurrent, pruritic follicular papules primarily affecting the trunk and proximal extremities. It predominantly occurs in young adults with dark skin tones, particularly in hot and humid climates, and is often chronic with variable responsiveness to treatment.
What is Disseminate and Recurrent Infundibulofolliculitis?
DRIF, first described in 1968 by Hitch and Lund, presents as monomorphic, pruritic papules pierced by hair follicles, typically 1-3 mm in size. These lesions are irregularly shaped and can be asymptomatic or mildly itchy, with aggravation by hot showers and relief from cool showers or emollients. The condition is more prevalent in Black or Negroid populations but has been reported across ethnicities.
The eruption often starts on the anterior neck, spreading to the lateral neck, upper chest, shoulders, back, and upper arms over 8-10 weeks. Despite its name, recurrence is not universal; many cases persist chronically before self-resolving after several years. There are no serious systemic consequences beyond cosmetic concerns and itch.
Who Gets Disseminate and Recurrent Infundibulofolliculitis?
This condition mainly affects young, healthy individuals with skin of color, such as Black men and women. It is uncommon overall but underreported due to its often asymptomatic nature. Cases have been noted in patients without atopy history, though some report familial or personal atopic backgrounds. Hot, humid environments exacerbate onset, suggesting environmental triggers.
- Demographics: Predominantly Black/Negroid adults, young age group.
- Risk Factors: Dark skin, hot/humid climates, possible genetic predisposition.
- Prevalence: Rare; exact incidence unknown due to underreporting.
Clinical Features
Lesions appear as discrete, follicular papules, 1-2 mm in diameter, pierced by a hair shaft. They are flesh-colored or hypopigmented on dark skin, sometimes progressing to pustules or lichenification with chronic rubbing. Distribution is along neck creases, upper trunk, shoulders, and proximal extremities; face, genitals, or lower limbs are rarely involved.
Itch varies from absent to intense, worsened by heat and humidity. Some patients note simultaneous onset in peers, hinting at shared environmental factors. Xerosis (dry skin) may accompany lesions without hand dermatitis or atopy signs.
| Feature | Description | Frequency |
|---|---|---|
| Papules | 1-3 mm follicular, monomorphic | Universal |
| Pruritus | Mild to severe, heat-aggravated | Common (variable) |
| Pustules | Scattered 1-2 mm | Occasional |
| Lichenification | From chronic scratching | In persistent cases |
| Distribution | Neck, trunk, upper arms | Typical |
Diagnosis
Diagnosis relies on clinical presentation and histopathology from skin biopsy, as no specific lab tests exist. Direct immunofluorescence is negative, ruling out autoimmune conditions.
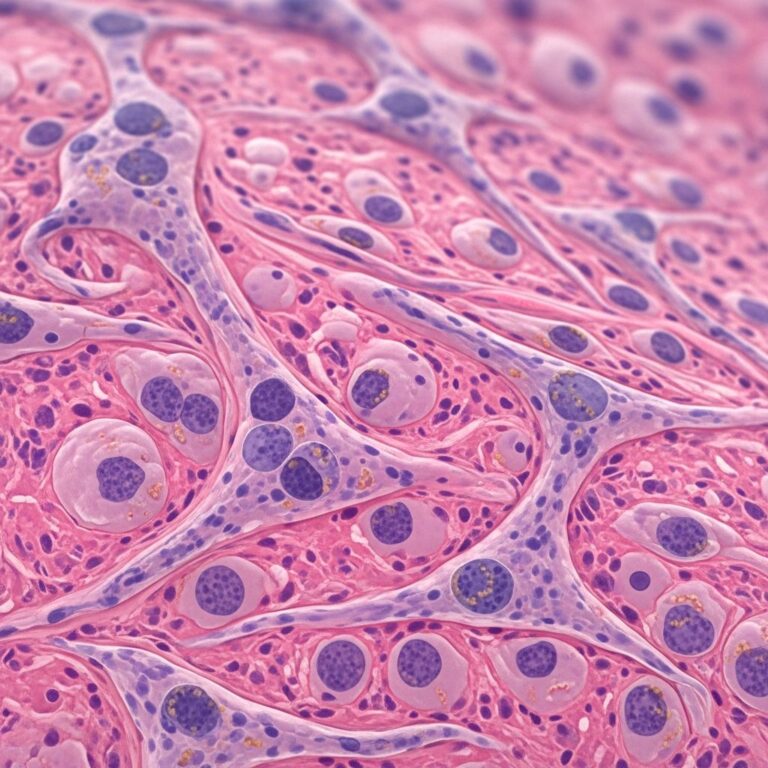
Histopathology
Key findings include perifollicular mononuclear (lymphocytic) infiltrate concentrated around the infundibulum (upper follicle). There is oedema, spongiosis (minimal to marked), widened follicular ostia, and basal layer involvement. Dermal melanophages, hyperkeratosis, or parakeratosis may occur, but no organisms or significant epidermal changes elsewhere.
- Hallmark: Lymphocytic infiltration at infundibulum.
- Variants: Spongiosis, exocytosis, fibrinoid necrosis (rare).
- Negative: Fungal elements, bacteria, marked hyperkeratosis.
Differential Diagnosis
DRIF mimics several folliculocentric eruptions. Key differentiators include histopathology and clinical course.
| Condition | Key Features | Distinguishing from DRIF |
|---|---|---|
| Papular Eczema | Atopic history, spongiosis, seasonal itch | No atopy, infundibulum-specific infiltrate |
| Keratosis Pilaris | Hyperkeratosis, rough feel | No hyperkeratosis histologically |
| Bacterial Folliculitis | Pus, responds to antibiotics | No bacteria, treatment-resistant |
| Pityrosporum Folliculitis | Fungal elements, trunk | No yeast on biopsy |
| Lichen Planus Follicularis | Polygonal papules, mucosal involvement | No Wickham striae, infundibular focus |
Causes and Pathophysiology
Etiology is unknown; infectious (bacterial/fungal) theories are unlikely due to absent organisms and non-response to antimicrobials. Possible links to atopy, occlusion, or follicular hyperproliferation exist, but no definitive cause. Hot/humid climates suggest environmental role, perhaps sweat-induced irritation.
Treatment
DRIF is often treatment-resistant but self-limited. No standard therapy; options are anecdotal with varying success. Retinoids show promise.
- First-line: Cooling emollients, avoid heat/humidity.
- Topical: Potent steroids (e.g., fluocinonide 8 weeks, then maintenance); tretinoin 0.025% (2 weeks resolution reported).
- Systemic: Isotretinoin, high-dose vitamin A, doxycycline (limited efficacy).
- Phototherapy: PUVA, narrow-band UVB (moderate benefit).
- Others: Tacrolimus, vitamins A/E, antihistamines (variable).
One case achieved 1-year remission with fluocinonide; another resolved promptly with tretinoin. Pregnant patients may opt for observation.
Prognosis and Complications
Benign, resolves spontaneously in years. Chronic cases may scar from lichenification. No systemic risks; management focuses on symptom relief and cosmesis.
Frequently Asked Questions (FAQs)
Is disseminate and recurrent infundibulofolliculitis contagious?
No, it is not infectious and does not spread person-to-person.
Does DRIF always recur?
Not necessarily; many cases persist chronically but resolve without recurrence after years.
Can DRIF affect light-skinned individuals?
Primarily dark skin, but cases reported in other ethnicities.
What triggers DRIF outbreaks?
Hot, humid conditions and showers; exact triggers unknown.
Is biopsy always needed for diagnosis?
Often yes, to confirm histopathology and exclude mimics.
References
- Disseminate and recurrent infundibulofolliculitis: A case — eScholarship. 2005. https://escholarship.org/uc/item/9ct798f5
- Disseminate and Recurrent Infundibulofolliculitis – PMC — PubMed Central. 2019-09-25. https://pmc.ncbi.nlm.nih.gov/articles/PMC6749767/
- Successful treatment of infundibulofolliculitis with topical tretinoin — Our Dermatology Online. 2012. https://www.odermatol.com/wp-content/uploads/file/2012%203/DOI-12.pdf
- Disseminate and recurrent infundibulofolliculitis — Wikipedia (background). N/A. https://en.wikipedia.org/wiki/Disseminate_and_recurrent_infundibulofolliculitis
- Disseminate and recurrent infundibulofolliculitis — DermNet NZ. Recent update. https://dermnetnz.org/topics/disseminate-and-recurrent-infundibulofolliculofolliculitis
- Disseminate and Recurrent Infundibular Folliculitis — PubMed Central. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC10986870/
Similar Articles






Read full bio of Sneha Tete