Escherichia coli O157:H7 Infection: Causes, Symptoms & Treatment
Understanding E. coli O157:H7: symptoms, transmission, diagnosis, and evidence-based treatment strategies.

Escherichia coli O157:H7 Infection: A Comprehensive Overview
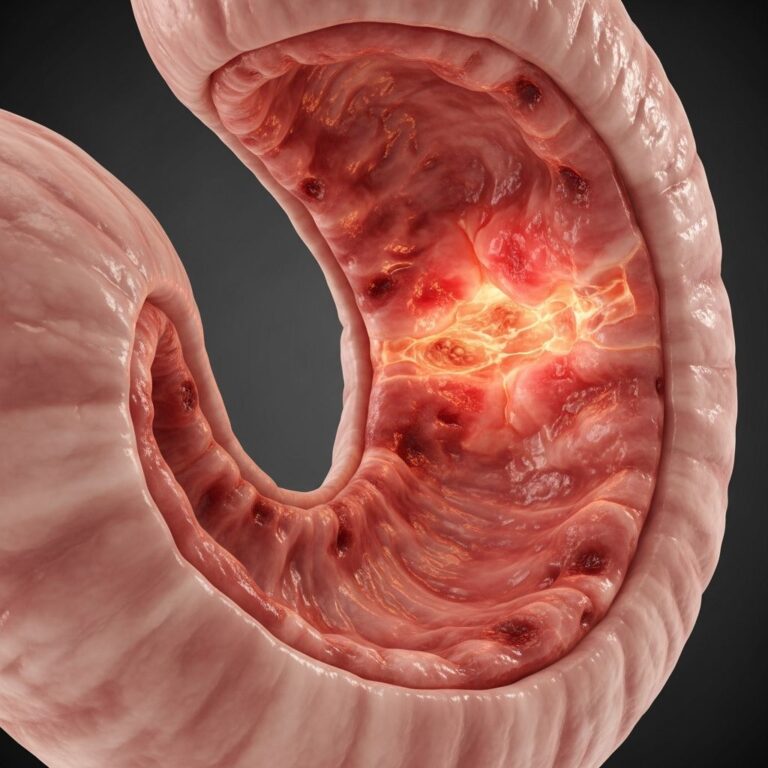
Escherichia coli O157:H7 is a potentially serious gram-negative bacterium that produces powerful toxins capable of causing severe gastrointestinal illness and life-threatening complications. This strain belongs to a group of enterohemorrhagic E. coli (EHEC) known for producing Shiga toxins that directly damage the intestinal lining and vascular endothelial cells. Unlike most E. coli strains that are harmless or cause only mild gastrointestinal distress, O157:H7 has emerged as a significant public health concern, particularly in developed nations where it is a leading cause of bacterial foodborne illness.
How E. coli O157:H7 Infection Occurs
Infection with E. coli O157:H7 typically results from the consumption of contaminated food or water. The most commonly reported sources include undercooked ground beef, raw milk, contaminated produce, and other foods exposed to fecal matter during processing or preparation. The bacteria can survive in the intestinal tract of infected individuals and animals, making cross-contamination a significant transmission pathway. Once ingested, the pathogenic bacteria colonize the large intestine where they produce high levels of Shiga toxins that are structurally similar to the potent cytotoxins produced by Shigella dysenteriae type 1.
The incubation period—the time between exposure and symptom onset—typically ranges from three to four days, although symptoms may appear as early as one day after exposure or as late as one to two weeks following initial contact with the bacterium. This variable incubation period makes it challenging for individuals to accurately identify the source of infection.
Symptoms and Clinical Presentation
E. coli O157:H7 infection typically begins acutely with distinctive gastrointestinal symptoms. The characteristic presentation includes:
– Severe abdominal cramps and pain- Watery diarrhea that may become grossly bloody within 24 hours- In some cases, patients report diarrhea as being “all blood and no stool,” a condition termed hemorrhagic colitis- Nausea and vomiting in some individuals- Minimal or absent fever (typically absent or low-grade, occasionally reaching 39°C or 102°F)
In uncomplicated infections, diarrhea typically lasts between one to eight days. Most people experience mild to moderate symptoms that resolve without serious complications, though the severity can vary considerably between individuals. Some infected persons may remain asymptomatic while still carrying and shedding the bacteria in their stool, making them potential sources of transmission to others.
Risk Factors and Vulnerable Populations
While anyone can become infected with E. coli O157:H7, certain populations face significantly elevated risk of severe illness and complications. Children under five years of age are particularly vulnerable due to their developing immune systems and smaller body mass. The elderly population similarly experiences increased susceptibility to serious complications. Immunocompromised individuals, including those with HIV/AIDS or those undergoing immunosuppressive therapy, face heightened risk of severe infection.
Seasonal variations in infection rates have been documented, with cases occurring more frequently during summer months when outdoor food preparation and consumption increase the likelihood of contamination and exposure. Understanding these risk factors is essential for targeted prevention and early intervention strategies.
Diagnosis and Laboratory Testing
Accurate diagnosis of E. coli O157:H7 infection requires specific laboratory testing, as clinical symptoms alone cannot definitively confirm the presence of this particular strain. The primary diagnostic methods include:
– Stool culture: Traditional bacterial culture remains a standard diagnostic approach, though it requires several days for results.- Shiga toxin assay: Rapid immunological testing for Shiga toxin or toxin-producing genes in stool samples- Molecular testing: Polymerase chain reaction (PCR) and other molecular techniques can identify specific genes encoding Shiga toxins, often providing faster results than traditional culture
A rapid stool assay for Shiga toxin or molecular testing for the gene encoding the toxin can facilitate immediate diagnosis, though positive results must be interpreted within the appropriate clinical context. Healthcare providers often distinguish E. coli O157:H7 from other conditions by noting that characteristically, no inflammatory cells are found in the stool fluid, helping differentiate this infection from inflammatory bowel disease or other intestinal inflammatory conditions.
Potential Complications
While most E. coli O157:H7 infections resolve without serious complications, a concerning subset of patients develop potentially life-threatening complications. The most significant complication is hemolytic-uremic syndrome (HUS), which occurs when the infection leads to systemic toxin absorption affecting vascular endothelial cells throughout the body, particularly in the kidneys.
Hemolytic-Uremic Syndrome (HUS)
Hemolytic-uremic syndrome represents the most serious complication of E. coli O157:H7 infection, developing in approximately 2 to 7 percent of infected individuals. This life-threatening condition involves:
– Hemolytic anemia (destruction of red blood cells)- Thrombocytopenia (severe reduction in platelet count)- Acute kidney injury or failure- Rapid fall in hematocrit levels- Elevated serum creatinine indicating renal dysfunction- Hypertension and possible signs of fluid overload- Bleeding diathesis (increased bleeding tendency)- Neurologic symptoms and complications
Children under five years of age experience the highest risk of developing HUS, and in the United States, HUS caused by E. coli O157:H7 is the leading cause of acute kidney failure in children. Patients who develop HUS typically require intensive care hospitalization, including dialysis and other specific supportive therapies, often at tertiary medical centers equipped to manage these critical complications.
Other Complications
Beyond HUS, patients may experience thrombotic thrombocytopenic purpura (TTP), another serious thrombotic microangiopathy requiring hospitalization for blood transfusions and supportive care. Additionally, chronic colonization with E. coli O157:H7 can occur after resolution of acute symptoms, potentially resulting in reinfection or transmission to other individuals.
Treatment Approach and Management Strategy
The management of E. coli O157:H7 infection is primarily supportive rather than antimicrobial. This approach represents a significant departure from treatment strategies for many other bacterial infections and reflects decades of clinical experience and scientific evidence.
Supportive Care
The mainstay of treatment for EHEC infection is supportive care focused on maintaining hydration and electrolyte balance. Fluid and electrolyte replacement represents the cornerstone of management, whether through oral rehydration solutions or intravenous fluids in severe cases. Most patients recover without specific antimicrobial treatment within five to ten days. Careful monitoring of vital signs, fluid intake and output, and clinical symptoms ensures early detection of complications.
What NOT to Use: Critical Safety Considerations
Several treatment approaches once considered standard are now contraindicated in E. coli O157:H7 infection:
– Antibiotics are not recommended: Despite the bacteria’s sensitivity to most commonly used antibiotics, antibiotic therapy has not been shown to alleviate symptoms, reduce bacterial carriage, or prevent hemolytic-uremic syndrome development. More concerning, antibiotics may precipitate HUS by triggering prophage induction, causing infected bacteria to release Shiga toxins more rapidly and convert other susceptible bacteria into toxin-producing forms.- Fluoroquinolones should be avoided: These antibiotics are specifically suspected of increasing the release of enterotoxins and significantly elevating the risk of hemolytic-uremic syndrome development.- Antidiarrheal agents are contraindicated: Medications such as loperamide (Imodium) and other antimotility agents should not be administered, as they increase the risk of systemic complications and may prolong infection duration by allowing toxins to remain in the intestinal tract longer.
High-Risk Patient Monitoring
In the first two weeks following infection, patients at high risk of developing hemolytic-uremic syndrome—particularly children under five years and older adults—require close clinical observation for early signs of complications. Healthcare providers monitor for hemolytic anemia, thrombocytopenia, proteinuria, hematuria, red cell casts, and rising serum creatinine levels. Later complications including edema and hypertension warrant escalation of care.
Prevention Strategies
Preventing E. coli O157:H7 infection requires a multi-faceted approach emphasizing food safety, personal hygiene, and environmental sanitation:
– Cook ground beef to an internal temperature of 160°F (71°C) throughout- Avoid consuming raw or unpasteurized milk and milk products- Practice thorough hand hygiene, especially after bathroom use or handling animals- Wash fresh produce under running water before consumption- Prevent cross-contamination by using separate cutting boards for raw meat and other foods- Maintain proper sanitation standards in food preparation areas- Practice good hygiene when caring for infected individuals to prevent secondary transmission
Disease Progression and Resolution
In adults, E. coli O157:H7 infections generally resolve within one week without intervention. However, children infected with this bacterium present a different pattern, with approximately one-third continuing to carry and shed the organism in their stool for up to three weeks, even after clinical symptoms have resolved. This extended shedding period in children highlights the importance of stringent hygiene practices and infection control measures in household and childcare settings.
When to Seek Medical Attention
Individuals should seek prompt medical evaluation if they experience:
– Bloody diarrhea lasting more than a few days- Severe abdominal pain and cramping- Signs of dehydration (decreased urination, extreme thirst, weakness)- High fever- Vomiting that prevents fluid intake- Symptoms in very young children, elderly individuals, or immunocompromised persons- Any signs of kidney dysfunction or neurological symptoms
Frequently Asked Questions
Q: How quickly do symptoms appear after eating contaminated food?
A: Symptoms typically appear three to four days after exposure, but can range from one day to two weeks. This variable incubation period makes identifying the contamination source challenging.
Q: Is there a cure for E. coli O157:H7 infection?
A: There is no specific cure; treatment is supportive. Most infections resolve on their own within five to ten days with appropriate fluid management and monitoring.
Q: Why shouldn’t antibiotics be used?
A: Antibiotics may actually increase the risk of hemolytic-uremic syndrome by triggering release of Shiga toxins from dying bacteria, converting this into a more dangerous infection.
Q: Who is most at risk for serious complications?
A: Children under five years, elderly individuals, and immunocompromised persons face the highest risk of developing hemolytic-uremic syndrome and other serious complications.
Q: Can infected individuals transmit the bacteria to others?
A: Yes, infected individuals can transmit E. coli O157:H7 through direct contact, particularly if proper hand hygiene is not maintained. Children may shed bacteria in stool for up to three weeks.
Q: What should I do if I suspect E. coli O157:H7 infection?
A: Contact your healthcare provider for proper diagnosis through stool testing. Maintain hydration, avoid antibiotics and antidiarrheal medications, and seek urgent care if experiencing severe symptoms or signs of dehydration.
References
- Infection by Escherichia coli O157:H7 and Other Enterohemorrhagic E. coli (EHEC) — MSD Manuals. 2024. https://www.msdmanuals.com/professional/infectious-diseases/gram-negative-bacilli/infection-by-escherichia-coli-o157-h7-and-other-enterohemorrhagic-e-coli-ehec
- E. coli – Symptoms and Causes — Mayo Clinic. 2023. https://www.mayoclinic.org/diseases-conditions/e-coli/symptoms-causes/syc-20372058
- E. coli O157:H7 Infections — Wisconsin Department of Health Services. 2024. https://www.dhs.wisconsin.gov/publications/p4/p42044.pdf
- Shiga toxin-producing Escherichia coli infection — Centre for Health Protection, Hong Kong Department of Health. 2024. https://www.chp.gov.hk/en/healthtopics/content/24/23315.html
- About Escherichia coli Infection — Centers for Disease Control and Prevention. 2024. https://www.cdc.gov/ecoli/about/index.html
Similar Articles






Read full bio of medha deb