Folliculosebaceous Cystic Hamartoma Pathology
Detailed pathology of folliculosebaceous cystic hamartoma: a rare cutaneous hamartoma with epithelial and mesenchymal features.

Folliculosebaceous cystic hamartoma (FSCH) is a rare benign cutaneous hamartoma characterized by a disorganized mix of epithelial and mesenchymal elements, primarily centered in the dermis. First described in 1991, it typically manifests as papules or nodules on the face and scalp of adults.
Definition / typical histology
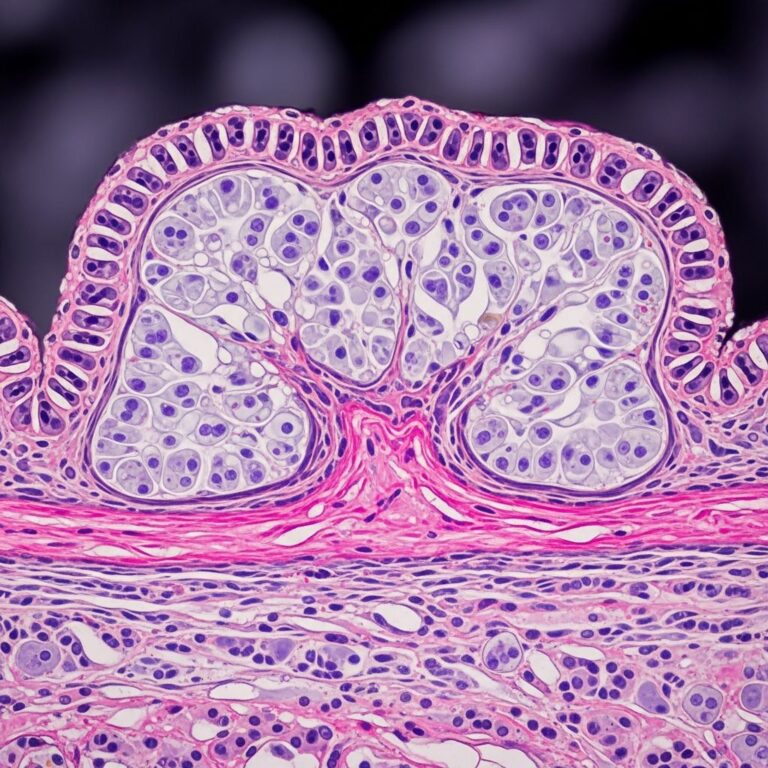
Folliculosebaceous cystic hamartoma represents a biphasic hamartoma combining distorted folliculosebaceous units with mesenchymal stroma. The epithelial components feature cystically dilated follicular infundibula filled with keratin, surrounded by radiating lobules of mature sebaceous glands. Mesenchymal elements include fibroplasia, vascular proliferation, and adipose tissue.
Scanning magnification reveals one or more dilated follicular structures with attached sebaceous lobules emanating radially, resembling a “spoke-wheel” pattern. The cystic cavity shows infundibular keratinization with a prominent granular layer but lacks hair shafts. Surrounding stroma exhibits dense collagen bundles, often with clefting from adjacent dermis, increased vascularity, and adipocytic clusters.
- Epithelial features: Infundibular cyst with keratin debris, thin anastomosing epithelial strands, hyperplastic sebaceous lobules.
- Mesenchymal features: Fibrous stroma, vascular channels, adipocytes; clefting at epithelial-stromal interface.
Immunohistochemistry is generally not required but may highlight epithelial components (pancytokeratins) and mesenchymal elements (CD34 for vessels, factor XIIIa for fibroblasts).
Pathogenesis
The exact pathogenesis of FSCH remains unclear, with debates on whether it constitutes a distinct entity or a variant within the trichofolliculoma spectrum. Proposed mechanisms include:
- Abnormal folliculosebaceous unit development during embryogenesis, leading to hamartomatous proliferation.
- Secondary mesenchymal changes in pre-existing sebaceous trichofolliculoma (STF), such as stromal fibrosis and cyst dilation from follicular regression.
- Associations with melanocytic nevi (e.g., Miescher-type) in 4.6% of cases, suggesting nevus-induced epithelial induction.
Rare reports link FSCH to neurofibromatosis type I, though likely incidental due to differing cellular origins. Over 150 cases documented, predominantly sporadic without genetic associations identified.
Clinical features
FSCH presents as solitary, skin-colored to yellowish papules or nodules (3-10 mm) with slow growth. Predilection sites include central face (nose 40-50%), eyelids, cheeks, scalp; less commonly trunk, extremities, genitals, or nipple.
| Demographics | Details |
|---|---|
| Age | 4-84 years; peak middle-aged/elderly (mean ~50). |
| Sex | Male predominance (1.5:1 M:F ratio). |
| Size | 2-15 mm diameter; protruding, non-tender. |
| Symptoms | Asymptomatic; rare ulceration or hair tufting. |
Lesions mimic basal cell carcinoma, sebaceous hyperplasia, or cysts clinically, necessitating biopsy.
Pathology description
Scanning view
Low-power examination shows a well-circumscribed dermal nodule with central cystic space(s) rimmed by sebaceous lobules. Stroma is paucicellular, collagenous, with artifactual clefts separating it from normal dermis (key diagnostic clue).
Cytology descriptions
- Cystic structure: Lined by stratified squamous epithelium with granular layer; filled with laminated keratin, no vellus hairs or primitive follicles.
- Sebaceous lobules: Mature, with peripheral germinative cells transitioning to sebocytes; no atypia.
- Stroma: Dense hyalinized collagen, dilated capillaries, mature adipocytes (10-30% in some cases); occasional spindle cells.
Other histology descriptions
Variants include:
- Prominent lipomatous stroma (adipose-rich FSCH).
- Spindle cell proliferation mimicking lipoma.
- Nevus-associated: Junctional melanocytes at epithelial-stromal interface.
- Rare anetodermic changes or ulceration.
No mitoses, atypia, or necrosis; benign throughout.
Differential diagnosis
Key mimics include:
| Entity | Distinguishing Features from FSCH |
|---|---|
| Sebaceous trichofolliculoma (STF) | Epidermal connection; hair shafts/vellus follicles in cyst; less stromal clefting/mesenchymal change. Clinically depressed with hairs. |
| Trichofolliculoma | Multiple small follicles budding into central dilated follicle; minimal sebaceous component; no adipocytes. |
| Steatocystoma | Smooth cyst wall without attached glands; no mesenchymal stroma; often multiple. |
| Dermoid cyst | Adnexal differentiation (sweat glands); deeper subcutaneous location; possible bone/cartilage. |
| Neurofibroma | Spindled Schwann cells (S100+); no cystic/sebaceous elements; plexiform in NF1. |
| Basaloid neoplasms | Atypia/mitoses; peripheral palisading (BCC); no sebaceous lobules. |
FSCH distinguished by triad: infundibular cyst + radiating sebaceous lobules + mesenchymal stroma with clefting.
Pathology images
(Image descriptions based on typical histology; actual images show:)
- Fig 1: Scanning view of dilated follicle with sebaceous lobules and clefted stroma.
- Fig 2: Higher power of keratin-filled cyst and mature sebocytes.
- Fig 3: Anastomosing epithelial cords in fibrous stroma.
- Fig 4: Adipocytic pockets and vascularity in mesenchyme.
References
References
- Folliculosebaceous Cystic Hamartoma in a Patient with Neurofibromatosis Type I — PMC/NCBI. 2011-11-15. https://pmc.ncbi.nlm.nih.gov/articles/PMC3229061/
- Folliculosebaceous cystic hamartoma pathology — DermNet NZ. 2023. https://dermnetnz.org/topics/folliculosebaceous-cystic-hamartoma-pathology
- A clinicopathologic study of folliculosebaceous cystic hamartoma — PubMed. 2010-10. https://pubmed.ncbi.nlm.nih.gov/20885285/
- Folliculosebaceous cystic hamartoma with spindle cell lipoma — Ovid/Journal of Cutaneous Pathology. 2014-02. https://www.ovid.com/journals/jcup/fulltext/00004735-201402000-00382~folliculosebaceous-cystic-hamartoma-with-spindle-cell
- Clinicopathological and immunohistochemical findings in a series of folliculo-sebaceous cystic hamartoma — Wiley Online Library. 2008. https://onlinelibrary.wiley.com/doi/10.1111/j.1600-0560.2008.01011.x
Frequently Asked Questions (FAQs)
Q: What is folliculosebaceous cystic hamartoma?
A: FSCH is a benign hamartoma of skin adnexa featuring cystic follicular structures, sebaceous glands, and mesenchymal stroma, typically on the face.
Q: How is FSCH diagnosed?
A: Primarily by histopathology showing the characteristic triad of infundibular cyst, radiating sebaceous lobules, and clefted stroma.
Q: Is FSCH malignant?
A: No, it is entirely benign with no atypia or malignant potential reported.
Q: What is the treatment for FSCH?
A: Complete surgical excision for diagnosis and cosmesis; no recurrence post-excision.
Q: How does FSCH differ from sebaceous trichofolliculoma?
A: FSCH lacks epidermal connection and hair shafts, shows more mesenchymal changes and clefting; STF has hairs and epidermal continuity.
Similar Articles






Read full bio of medha deb