Fox-Fordyce Disease: Symptoms, Causes, and Treatment
Complete guide to Fox-Fordyce disease: Understanding apocrine miliaria, diagnosis, and management strategies.

Fox-Fordyce Disease: A Comprehensive Overview
Fox-Fordyce disease, also known as apocrine miliaria, is a rare chronic inflammatory skin disorder that affects the apocrine sweat glands. This condition is characterized by the entrapment of apocrine sweat, resulting in inflammation and a distinctive pruritic papular eruption. First described in 1902 by George Henry Fox and John Addison Fordyce, the disease predominantly affects women and significantly impacts quality of life due to intense itching and visible skin changes. The condition typically develops in areas where apocrine glands are concentrated, including the axillae (underarms), anogenital regions, and periareolar areas.
Understanding the Etiology and Pathophysiology
While the exact etiology of Fox-Fordyce disease remains unclear, obstruction of the apocrine gland duct due to keratin accumulation is believed to play a central role in disease development. The pathophysiology involves a complex series of events within the apocrine gland system.
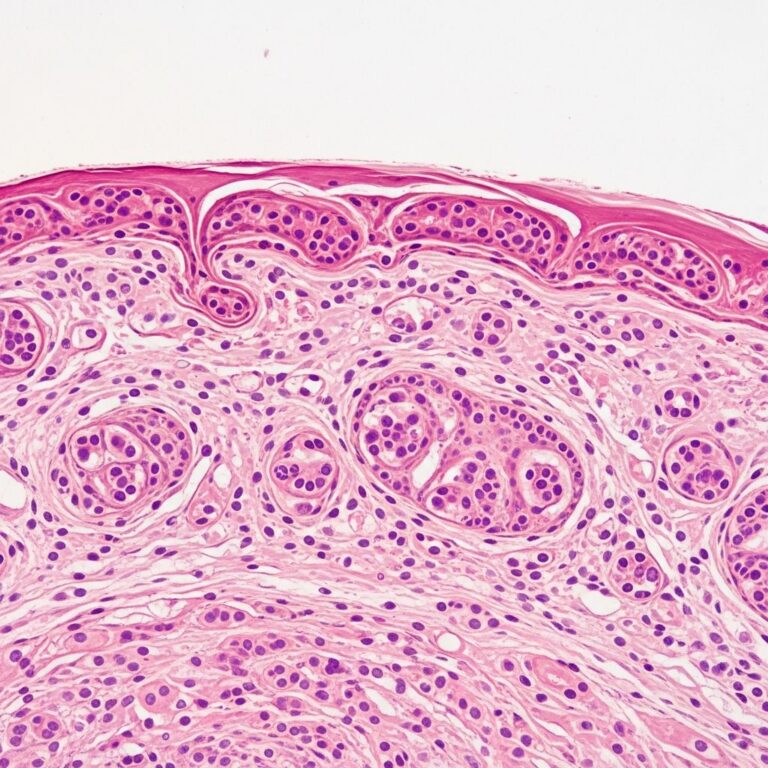
Histopathological examination typically reveals characteristic findings that aid in diagnosis. These include hyperkeratosis (thickened outer skin layer) and plugging of the apocrine gland’s follicular infundibulum and excretory duct. As apocrine secretions accumulate proximal to the plug within the dilated duct, a spongiotic vesicle may form, potentially leading to duct rupture. The resulting inflammation is characterized by perifollicular infiltration of lymphocytes and foamy histiocytes, often resulting in hair loss in affected areas.
The disease follows a relapsing-remitting course, meaning it goes through phases of improvement and worsening over time. Certain triggers, such as excessive sweating, heat, stress, and anxiety, can exacerbate symptoms and precipitate disease flares.
Clinical Presentation and Symptoms
The characteristic presentation of Fox-Fordyce disease includes several distinctive clinical features that help distinguish it from other dermatological conditions. The primary complaint in affected individuals is
severe and persistent pruritus
(itching), which can be exacerbated by hyperhidrosis (excessive sweating), sweating in general, stress, and anxiety.Common clinical signs include:
- Numerous small, flesh-colored to slightly erythematous papules (small bumps)
- Localization to apocrine gland-bearing areas, particularly the axillae (underarms), anogenital regions, and periareolar areas
- Intense and chronic itching that significantly impacts quality of life
- Hyperhidrosis or excessive sweating in affected regions
In chronic cases, repeated scratching can lead to secondary skin changes. These include lichenified (thickened and leathery), coarse, and hyperpigmented skin as a result of chronic trauma and inflammation. Severe cases may manifest with localized anhidrosis (decreased sweating) and brittle, sparse, or absent hair due to destruction of glands and hair follicles. Secondary bacterial infections may occur as a complication of persistent scratching, manifesting as oozing and crusting over lesions.
Diagnostic Approaches
Diagnosis of Fox-Fordyce disease is primarily made clinically based on characteristic history, clinical appearance, and physical examination findings. The disease is usually diagnosed on the history and clinical appearance of the rash, as there are no specific diagnostic tests available.
Healthcare providers assess for the typical localization, uniform appearance, and symptomatology characteristic of the condition. The major clinical signs used in diagnosis include chronic pruritus and numerous small papules around the axillae, genitalia, and periareolar regions.
Skin Biopsy: While clinical diagnosis is often sufficient, a skin biopsy may be performed to confirm the diagnosis or rule out other conditions, particularly when clinical findings are unclear. An experienced dermatopathologist is necessary to correctly diagnose the disease from a biopsy. The biopsy may require serial sectioning to demonstrate the characteristic histological findings. Histologic hallmarks include hyperkeratosis of the epidermis with follicular plugging and intermittent spongiosis, rupture of the apocrine gland, and chronic peri-infundibular or periductal lymphocytic or neutrophilic inflammation.
Differential diagnosis should exclude other conditions such as folliculitis, hidradenitis suppurativa, eczema, and other inflammatory skin disorders that may present similarly.
Treatment Options and Management Strategies
There is currently no definitive cure for Fox-Fordyce disease; however, symptomatic improvement to complete resolution has been reported with various treatment modalities. Treatment selection depends on disease severity, patient response, and individual tolerance. Management focuses on alleviating symptoms, particularly the intense pruritus, and preventing disease flares.
First-Line Treatment Approaches
First-line treatments are selected due to their availability, ease of administration, and low risk for serious adverse effects. However, there is no established optimal treatment regimen, and recurrence may occur upon cessation of treatment.
Topical Medications:
- Topical retinoids (tretinoin and adapalene) reduce follicular blockage and have demonstrated efficacy in managing symptoms
- Topical corticosteroids decrease inflammation and itching
- Topical clindamycin in alcoholic propylene glycol solution is effective as an anti-inflammatory agent
- Calcineurin inhibitors (such as pimecrolimus) reduce inflammation without the side effects of prolonged steroid use
- Benzoyl peroxide has been used with variable success
Oral Medications:
- Oral retinoids (isotretinoin) have demonstrated promising results in anecdotal reports
- Oral contraceptives may benefit hormonally-sensitive cases
- Antihistamines (such as loratadine) provide symptomatic relief from itching
- Hormonal therapy including estrogen hormones may help in appropriate candidates
Second-Line and Advanced Treatment Options
These treatments are reserved for severe and refractory cases unresponsive to first-line therapy. Advanced options include both surgical and laser-based approaches:
- Fractional lasers (1550 nm erbium-glass) to resurface affected areas
- Pulsed dye laser therapy
- Botulinum toxin (Botox) injections to reduce sweating and associated irritation, either to treat itch or excess sweating as a trigger
- Phototherapy using specialized light wavelengths
- Surgical excision of affected tissue
- Electrocoagulation and copper vapor laser
- CO2 laser treatment
- Liposuction-assisted curettage
- Microwave technology for targeted tissue ablation
- Laser hair removal to reduce hair follicle occlusion and apocrine gland activity
Lifestyle and Supportive Care
Non-pharmacological management is an important component of treatment strategy. Avoidance of excessive sweating may minimize disease flares significantly. Additional supportive measures include:
- Avoiding heat and friction in affected areas
- Using gentle, non-comedogenic personal care products
- Managing stress, which may worsen symptoms
- Wearing breathable, loose-fitting clothing
- Maintaining good hygiene to prevent secondary infections
Treatment Efficacy and Individual Response
The treatment of Fox-Fordyce disease is directed toward the specific symptoms apparent in each individual, and consultation with a dermatologist is recommended for optimal management. No single therapy is universally effective in all patients, highlighting the need for individualized treatment approaches. Specific therapies that have been used with variable degrees of success include estrogen hormones, oral retinoids, steroid creams, and topical antibiotics.
Nonsurgical treatment can be difficult because no single treatment has been shown to be universally very effective; however, avoidance of excessive sweating or heat remains a cornerstone of management. Patient outcomes depend on disease severity, trigger identification, treatment selection, and individual response patterns.
Prognosis and Long-Term Outlook
The overall prognosis for patients with Fox-Fordyce disease is relatively favorable, though challenging to predict on an individual basis. While there is currently no definitive cure, symptomatic improvement to complete resolution has been reported with the treatment modalities previously discussed.
The disease typically follows a chronic course with intermittent flares, and treatment is often difficult to manage consistently. However, with appropriate identification and avoidance of triggers, combined with targeted therapeutic interventions, many patients experience significant symptom reduction and improved quality of life. Regular follow-up with dermatology specialists ensures optimal management and early intervention when disease flares occur.
Frequently Asked Questions
Q: Is Fox-Fordyce disease contagious?
A: No, Fox-Fordyce disease is not contagious. It is a chronic inflammatory condition affecting individual apocrine glands and cannot be transmitted to other people through contact or other means.
Q: Can Fox-Fordyce disease affect men?
A: While Fox-Fordyce disease predominantly affects women, it can occasionally occur in men, though cases are much rarer. The reason for the female predominance is not fully understood.
Q: How long does treatment typically take to show results?
A: Treatment response varies by individual and therapy type. Some topical treatments may show improvement within 2-4 weeks, while others require longer courses of therapy. Oral medications and advanced procedures may require several weeks to months for noticeable improvement.
Q: Will Fox-Fordyce disease return after treatment?
A: Recurrence is possible upon cessation of treatment, as there is no permanent cure. However, many patients experience sustained improvement or long periods of remission with appropriate maintenance therapy and trigger avoidance.
Q: What triggers should I avoid?
A: Common triggers include excessive sweating, heat exposure, friction from clothing, stress, and anxiety. Identifying and avoiding personal triggers is crucial for minimizing disease flares and maintaining symptom control.
References
- Fox-Fordyce Disease (Apocrine Miliaria) – StatPearls — National Center for Biotechnology Information (NCBI Bookshelf). 2024. https://www.ncbi.nlm.nih.gov/books/NBK545207/
- Fox Fordyce Disease – Symptoms, Causes, Treatment — National Organization for Rare Disorders (NORD). 2024. https://rarediseases.org/rare-diseases/fox-fordyce-disease/
- Fox-Fordyce disease – BAD Patient Hub — British Association of Dermatologists Skin Health Info. 2024. https://www.skinhealthinfo.org.uk/condition/fox-fordyce-disease/
- Fox–Fordyce disease of the vulva — PubMed Central (PMC), National Institutes of Health. 2015. https://pmc.ncbi.nlm.nih.gov/articles/PMC4857685/
- Fox-Fordyce Disease (Apocrine Miliaria) — Dermatology Advisor. 2024. https://www.dermatologyadvisor.com/home/decision-support-in-medicine/dermatology/fox-fordyce-disease-apocrine-miliaria/
Similar Articles






Read full bio of Sneha Tete