Glomuvenous Malformation: Symptoms, Diagnosis & Treatment Guide
Understanding glomuvenous malformations: causes, symptoms, diagnosis, and effective treatment options for this rare vascular condition.

Glomuvenous malformation (GVM), also known as glomangioma or glomangiomatosis, is a rare vascular anomaly characterized by clusters of abnormal blood vessels and glomus cells in the skin and subcutaneous tissue. These lesions typically present as soft, pink, red, or bluish-purple nodules or plaques that are less compressible than typical venous malformations and often become painful over time.
Introduction
Glomuvenous malformations are congenital or arise in early childhood, distinguishing them from solitary glomus tumors, which are more common in adults and often subungual. Unlike common venous malformations, GVMs feature glomus cells—modified smooth muscle cells normally found in glomus bodies that regulate temperature via arteriovenous shunts. These lesions involve dilated venous channels lined by clusters of these glomus cells, leading to their unique appearance and symptoms.
GVMs can be sporadic or familial, with the latter following an autosomal dominant inheritance pattern linked to mutations in the GLMN gene on chromosome 1p21-22. This gene encodes glomulin, a protein that modulates vascular development; its loss-of-function leads to proliferation of glomus cells around venous structures.
Prevalence is low, with familial disseminated forms representing about 10% of cases. Lesions are multifocal in multiple GVMs, often affecting extremities, trunk, or segmental areas, and rarely mucous membranes or deeper structures.
Demographics
GVMs are typically diagnosed at birth, infancy, or childhood, though they may appear later. They affect both sexes equally and occur across ethnicities, with no strong racial predilection noted. Familial cases show vertical transmission, where 50% of offspring from an affected parent inherit the mutation.
In large cohorts, such as one reviewing 1685 patients with venous anomalies, GVMs were distinguished from cutaneomucosal venous malformations (VMCM) by genetic and clinical criteria. Sporadic cases mirror inherited ones in presentation but lack family history.
- Age of onset: Congenital (present at birth) or early childhood; progresses with age.
- Inheritance: Autosomal dominant in familial forms (~50% penetrance).
- Incidence: Rare; multiple lesions in <10% of glomus-related cases.
Clinical Features
GVMs manifest as localized, segmental, or disseminated collections of soft nodules or coalescing plaques, ranging from pink (in infants) to red, bluish-purple, or dark purple in adults. They are raised, often with a cobblestone-like, hyperkeratotic surface, and do not fully collapse on compression or elevation, unlike typical venous malformations.
Common sites include extremities (fingers, toes, arms, legs), trunk, and buttocks; rarely oral mucosa or eyelids. Lesions start painless but become tender to touch or pressure, especially if subungual. Pain worsens with age as lesions thicken, darken, and spread. Disseminated forms involve numerous (10-15+) nodules.
| Feature | Glomuvenous Malformation (GVM) | Venous Malformation (VM) |
|---|---|---|
| Color | Pink to bluish-purple/dark blue | Uniform blue |
| Compressibility | Partial; does not empty fully | Collapses with elevation/compression |
| Depth | Skin/subcutis; rarely muscle | Skin, mucosa, muscle, joints |
| Pain trigger | Pressure/touch | Activity, hormones, awakening |
| Surface | Cobblestone, hyperkeratotic | Smooth |
Progression: Lesions darken and hypertrophy over time; elastic garments may exacerbate pain in GVMs.
Diagnosis
Diagnosis relies on clinical evaluation of characteristic lesions: multiple, non-compressible, purple nodules on extremities. Doppler ultrasound reveals superficial venous components without deep flow. MRI confirms extent, showing hyperintense T2 lesions in skin/subcutis.
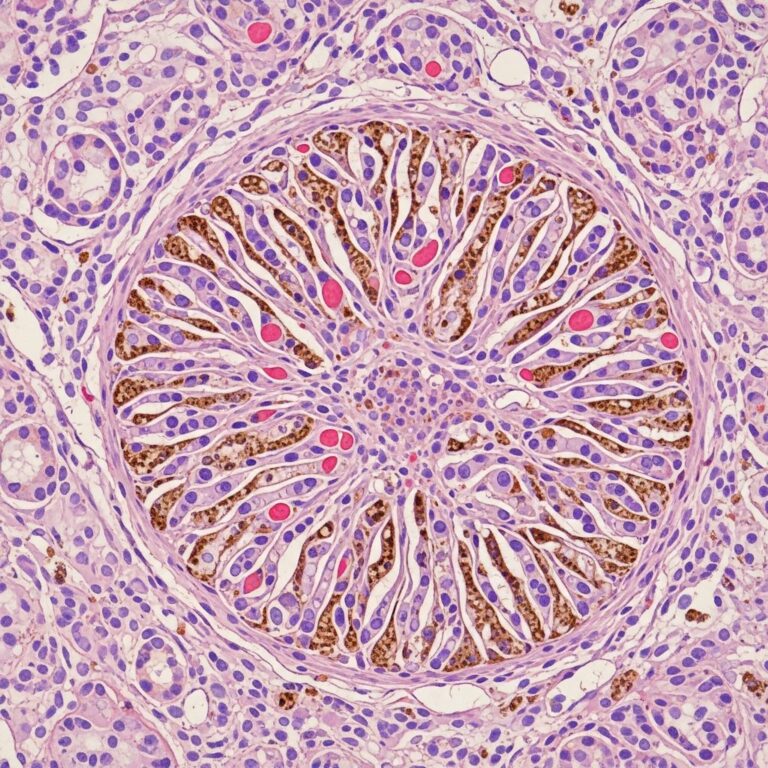
Histology is confirmatory: dilated, irregular venous channels in dermis/subcutis, lined by endothelium and surrounded by clusters of uniform, round glomus cells (alpha-smooth muscle actin positive, cuboidal nuclei). Unlike solid glomus tumors, GVMs lack encapsulation and have larger vascular spaces.
Genetic testing for GLMN mutations supports familial cases. Differential includes blue rubber bleb nevus syndrome, VMCM (TIE2 mutations), and solitary glomus tumors.
- Key histologic features: Ectatic vascular channels with glomus cells; acanthosis, papillomatosis.
- Imaging: US/MRI for venous nature; biopsy for differentiation.
Treatment
No cure exists; management is symptomatic and cosmetic. Options depend on lesion size, location, number, and symptoms.
Surgery: Most effective for localized lesions; excision or reconstructive plastic surgery yields good results.
Laser therapy: Pulsed dye or Nd:YAG lasers effective for small, flat, or plaque-like lesions, reducing color and pain.
Sclerotherapy: Indicated for accessible lesions; polidocanol foam or 96% ethanol gel (EU orphan drug for venous malformations) minimizes necrosis. Less risky than liquid ethanol.
Compression worsens pain, so avoided. Pain management with analgesics; monitor for complications like ulceration.
- Segmental/large: Combined surgery/sclerotherapy.
- Disseminated: Sequential laser/sclerotherapy.
- Observation: For asymptomatic cases.
Frequently Asked Questions (FAQs)
Q: Is glomuvenous malformation hereditary?
A: Yes, familial GVM follows autosomal dominant inheritance due to GLMN mutations, affecting 50% of offspring. Sporadic cases also occur.
Q: Are GVM lesions painful?
A: Initially painless, they often become tender to pressure over time, especially on extremities.
Q: How is GVM diagnosed?
A: By clinical appearance, confirmed with biopsy showing glomus cells, ultrasound, MRI, or genetic testing.
Q: What is the best treatment for multiple GVMs?
A: Sclerotherapy (polidocanol/ethanol) or laser for superficial lesions; surgery for larger ones.
Q: Do GVMs affect internal organs?
A: No, they are confined to skin/subcutis; rarely extend to muscle.
Prognosis and Complications
GVMs are benign but chronic, with cosmetic and pain impacts. Progression leads to thicker, darker lesions; rare ulceration or bleeding. Early intervention improves quality of life. Genetic counseling for familial cases.
References
- Orphanet: Glomuvenous malformation — Orphanet. 2023. https://www.orpha.net/en/disease/detail/83454
- Familial Disseminated Cutaneous Glomuvenous Malformation — PMC/NCBI. 2017-01-15. https://pmc.ncbi.nlm.nih.gov/articles/PMC5227083/
- Glomuvenous Malformations — Children’s Hospital of Philadelphia (CHOP). 2024. https://www.chop.edu/conditions-diseases/glomuvenous-malformations
- Glomuvenous malformation — DermNet NZ. 2023. https://dermnetnz.org/topics/glomuvenous-malformation
- Glomuvenous Malformation (Glomangioma) and Venous Malformation — JAMA Dermatology. 2006-11-01. https://jamanetwork.com/journals/jamadermatology/fullarticle/480721
- Glomuvenous malformations — Great Ormond Street Hospital (GOSH). 2024. https://www.gosh.nhs.uk/conditions-and-treatments/conditions-we-treat/glomuvenous-malformations/
Similar Articles






Read full bio of medha deb