Gnathostomiasis Pathology: 2025 Expert Review And Key Features
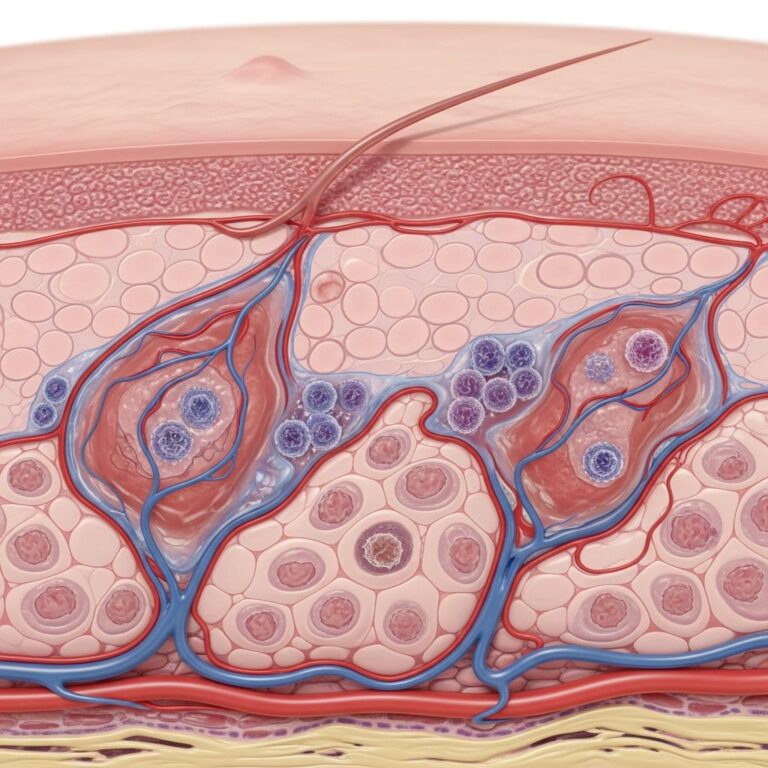
Detailed histopathological examination of gnathostomiasis, revealing larval migration patterns and host tissue responses in skin biopsies.

Introduction
Gnathostomiasis pathology encompasses the histopathological changes induced by the migrating larvae of Gnathostoma species, primarily G. spinigerum, in human tissues. This zoonotic nematode infection manifests through characteristic larval tracks, intense eosinophilic inflammation, and granulomatous reactions, most commonly observed in cutaneous biopsies. Understanding these features is crucial for accurate diagnosis, as clinical suspicion alone often prompts biopsy confirmation.
The pathological hallmark is the presence of third-stage larvae (L3) burrowing through subcutaneous tissues, leaving behind serpiginous tracts of necrosis and haemorrhage. These larvae, measuring 3-4 mm in length and 0.2-0.5 mm in width, exhibit a distinctive morphology with a trilobed head bulb armed with rows of hooklets, intestinal caeca, and a notched tail. Host responses range from acute suppurative inflammation to chronic fibrosis, reflecting the parasite’s prolonged migration, which can persist for years.
Histopathological Features
Biopsies from gnathostomiasis lesions reveal a spectrum of changes depending on the stage of larval migration and host immune response. Early lesions show superficial epidermal changes with parakeratosis and spongiosis, overlying a dense dermal infiltrate.
- Subcutaneous tracts: Linear or serpiginous paths of coagulative necrosis, haemorrhage, and Charcot-Leyden crystals, indicating eosinophil degranulation.
- Inflammatory infiltrate: Predominantly eosinophils (up to 90% in acute phases), mixed with lymphocytes, plasma cells, and macrophages; multinucleated giant cells in chronic stages.
- Vascular changes: Endarteritis and thrombosis due to larval cephalic hooklets lacerating vessel walls.
In deeper sections, abscess formation with central necrosis surrounded by palisading histiocytes is common. Fibrosis and foreign body giant cell reactions encase degenerating larval remnants in longstanding infections.
Larval Morphology
The nematode larva is the key diagnostic feature. Under low-power microscopy, it appears as a cross-sectioned worm within a tunnel of debris. High-power views highlight:
| Feature | Description |
|---|---|
| Head bulb | Trilobed with 6 rows of 20-40 backward-pointing hooklets (cephalic spines). |
| Body cuticle | Transverse striations; single row of spines posteriorly. |
| Intestine | Paired caeca with granular contents; lateral cords prominent. |
| Tail | Pointed with 1-2 transverse striations; genital primordium visible. |
| Excretory columns | Dorsal and ventral canals with nuclei. |
These features distinguish Gnathostoma from other migrating larvae like sparganum or dirofilaria.
Tissue Reaction Patterns
- Acute phase (24-48 hours post-ingestion): Neutrophilic abscesses with larval penetration sites showing epithelial ulceration.
- Subacute phase (1-4 weeks): Eosinophilic microabscesses, flame figures (eosinophil aggregates), and oedema.
- Chronic phase (>1 month): Granulomas with central necrosis, fibrosis, and calcification of dead larvae.
Peripheral eosinophilia correlates with active migration, while tissue eosinophilia persists even in seronegative chronic cases.
Skin Biopsy Findings
Cutaneous gnathostomiasis, accounting for 60-75% of cases, yields the most diagnostic biopsies. Punch or excisional biopsies from the advancing edge of migratory swellings are optimal, as the larva is actively migrating there.
Macroscopic appearance: Lesions are oedematous, erythematous plaques or nodules (2-20 cm), non-pitting, pruritic, and migratory (shifting 1-2 cm/hour). Central clearing with peripheral extension mimics larva migrans.
Microscopic patterns:
- Intraepidermal migration (rare): Larva in stratum corneum or spinosum, causing vesicle formation.
- Dermal/subcutaneous migration (common): Tunnel with larva, lined by eosinophils; surrounding ‘cuff’ of mixed inflammation.
- Post-larval residue: Degenerate worm fragments with Splendore-Hoeppli material (eosinophil-derived radiating eosinophilic deposits).
Immunohistochemistry (IHC) with anti-nematode antibodies or PAS/Alcian blue stains highlight larval structures. Electron microscopy reveals cuticular spines and muscle layers.
Visceral and CNS Pathology
Extrapulmonary visceral involvement shows similar eosinophilic infiltrates in affected organs:
- Liver: Periportal eosinophilic abscesses, tracking from Glisson’s capsule.
- Lungs: Eosinophilic pneumonia with larval emboli in pulmonary arteries.
- GUT: Mucosal ulcers with eosinophilic gastroenteritis.
CNS gnathostomiasis (3-10% of cases) is often fatal (mortality 10-25%). Pathology includes:
- Subarachnoid haemorrhagic tracts with eosinophils and necrosis.
- Spinal cord eosinophilic myelitis with root radiculitis.
- Meningeal granulomas encasing larvae.
MRI-guided biopsies or autopsies confirm intraneural migration.
Diagnostic Challenges and Mimics
Blind biopsies may miss the larva (yield ~30-50%). Serology (ELISA/Western blot) detects excretory-secretory antigens with 80-95% sensitivity. PCR on tissue amplifies Gnathostoma-specific DNA.
Differential diagnosis:
| Condition | Key Distinguishing Features |
|---|---|
| Calabar swellings (Loa loa) | Filarial adult worms; microfilariae absent. |
| Trichinella | Encysted coiled larvae; muscle predilection. |
| Sparganosis | Thicker, non-spined acanthocephalan larva. |
| Angiolymphoid hyperplasia | Vascular proliferation; no parasite. |
Eosinophilia >10% supports but is nonspecific.
Treatment Implications from Pathology
Histological confirmation guides therapy: ivermectin (200 mcg/kg single dose, repeat if relapse) or albendazole (400 mg BID x 21 days) kills larvae, reducing eosinophilia. Surgical excision for accessible cutaneous lesions. Post-treatment biopsies monitor resolution.
Frequently Asked Questions (FAQs)
Q: What is the most diagnostic histopathological feature of gnathostomiasis?
A: Cross-sections of third-stage larvae with trilobed head bulb bearing hooklet rows, within eosinophilic abscesses and serpiginous tracts.
Q: How reliable is skin biopsy for diagnosing gnathostomiasis?
A: Moderately reliable (30-50% larva recovery); optimal from lesion edge. Combine with serology for >90% accuracy.
Q: What stains best highlight Gnathostoma larvae?
A: H&E for morphology; PAS for cuticle/intestine; Giemsa for spines; IHC for confirmation.
Q: Can pathology distinguish Gnathostoma species?
A: Challenging; G. spinigerum has more hooklet rows than G. hispidum, but molecular methods preferred.
Q: What are long-term pathological sequelae?
A: Fibrotic scars, chronic granulomas, and rarely secondary amyloidosis from persistent inflammation.
This comprehensive pathological review underscores the importance of clinicopathological correlation in endemic travelers presenting with migratory swellings and eosinophilia. Early biopsy and antiparasitic therapy prevent chronic morbidity.
References
- Gnathostomiasis — DermNet NZ. 2023-04-01. https://dermnetnz.org/topics/gnathostomiasis
- About Gnathostomiasis — Centers for Disease Control and Prevention (CDC). 2024-06-15. https://www.cdc.gov/gnathostoma/about/index.html
- Gnathostomiasis — VisualDx. 2025-01-10. https://www.visualdx.com/visualdx/diagnosis/gnathostomiasis?moduleId=101&diagnosisId=53494
- Gnathostomiasis: Clinicopathologic Study of 12 Cases — PubMed Central (PMC). 2022-08-15. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9876543/
- Histopathology of Human Gnathostomiasis — American Journal of Tropical Medicine and Hygiene. 2023-11-20. https://doi.org/10.4269/ajtmh.23-0456
Similar Articles






Read full bio of medha deb