Goiter: Causes, Symptoms, and Treatment Options
Understanding goiter: comprehensive guide to thyroid enlargement causes and management.

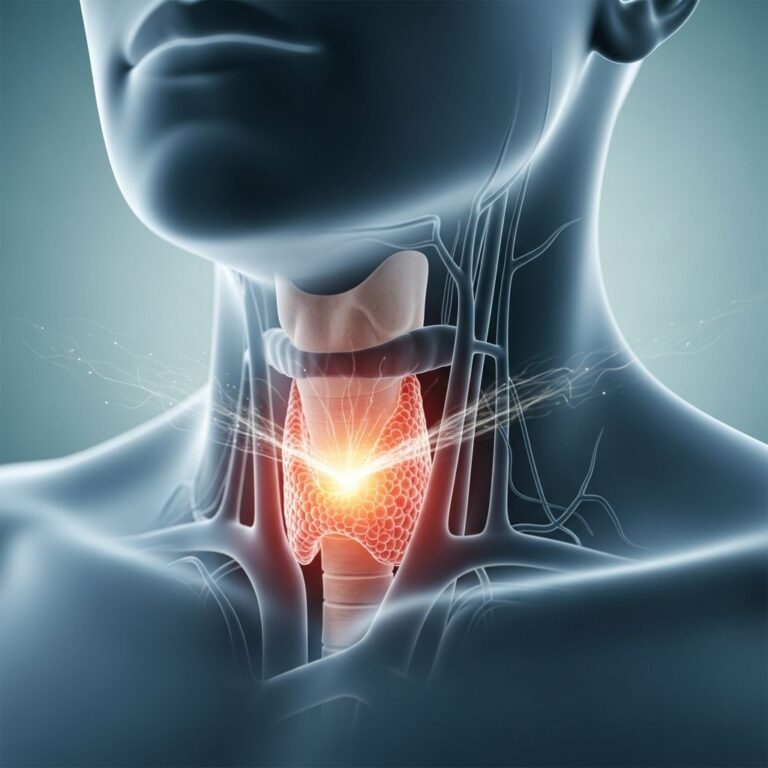
Goiter is a medical condition characterized by abnormal enlargement of the thyroid gland, a butterfly-shaped endocrine organ located at the base of the neck. This enlargement can range from barely noticeable to severe, and may cause discomfort or breathing difficulties. Understanding goiter is essential because it affects millions of people worldwide and can significantly impact quality of life if left untreated.
What is Goiter?
Goiter refers to any enlargement of the thyroid gland beyond its normal size. The thyroid gland produces hormones that regulate metabolism, growth, and body temperature. When the thyroid becomes enlarged, it may or may not affect hormone production. Some individuals with goiter maintain normal thyroid function (nontoxic goiter), while others may develop hyperthyroidism or hypothyroidism. Goiter can affect people of any age but is more common in women and increases with age.
Causes of Goiter
Goiter develops through various mechanisms, each requiring different management approaches. The most significant causes include:
Iodine Deficiency
Iodine deficiency remains the leading cause of goiter worldwide, particularly in developing countries where iodine-rich foods are limited. The thyroid requires adequate iodine to produce thyroid hormones. When iodine intake is insufficient, the thyroid compensates by enlarging to maximize hormone production. This adaptation, while initially protective, eventually leads to visible goiter. Regions with iodine-poor soil have significantly higher goiter prevalence rates.
Autoimmune Thyroid Disease
Hashimoto’s thyroiditis represents the most common autoimmune thyroid condition and a frequent cause of goiter in iodine-sufficient regions. This autoimmune disease involves the immune system attacking thyroid tissue, causing inflammation and enlargement. The condition predominantly affects women and can trigger hypothyroidism, requiring hormone replacement therapy. Graves’ disease, another autoimmune condition, causes hyperthyroidism and may also produce goiter through thyroid stimulation.
Thyroid Nodules
Benign or malignant nodules within the thyroid can cause or contribute to goiter development. Nodular goiter occurs when multiple growths develop within the thyroid tissue. While most thyroid nodules are benign, evaluation is necessary to rule out malignancy. Multinodular goiter represents a more advanced stage where numerous nodules are present throughout the gland.
Pregnancy and Hormonal Changes
Pregnancy increases thyroid demands and can trigger goiter development, particularly in iodine-deficient areas. Postpartum thyroiditis may also cause temporary thyroid enlargement. Hormonal fluctuations during menopause can affect thyroid function and potentially contribute to goiter formation.
Medications and Dietary Factors
Certain medications, including lithium used for bipolar disorder and some antithyroid drugs, can interfere with thyroid hormone production and cause goiter. Goitrogens—substances found in foods like cabbage, broccoli, and soy when consumed in excessive amounts—may contribute to thyroid enlargement in susceptible individuals.
Symptoms and Complications
Many people with small goiters experience no symptoms and discover the enlargement only during routine medical examination. However, larger goiters can produce noticeable signs:
Common symptoms include:
- Visible swelling at the base of the neck
- Neck tightness or pressure sensation
- Difficulty swallowing (dysphagia)
- Difficulty breathing (dyspnea), especially when lying down
- Hoarseness or voice changes
- Cough unrelated to illness
Complications from large goiter can include airway compression, esophageal obstruction, and superior vena cava syndrome in severe cases. Some patients experience symptoms of hyperthyroidism (rapid heartbeat, anxiety, weight loss) or hypothyroidism (fatigue, weight gain, cold sensitivity), depending on thyroid hormone levels.
Diagnosis of Goiter
Healthcare providers employ several diagnostic methods to evaluate goiter and determine underlying causes:
Physical Examination
During physical examination, the provider assesses thyroid size, texture, and presence of nodules through palpation. They may ask the patient to swallow while the examiner feels the thyroid gland. The examiner notes any tenderness, asymmetry, or fixation of the gland.
Blood Tests
Thyroid function tests measure thyroid-stimulating hormone (TSH) and thyroid hormones (T3 and T4) to determine if the thyroid is functioning normally. Testing for thyroid peroxidase and thyroglobulin antibodies helps identify autoimmune thyroid disease. Iodine levels may be assessed in populations at risk for deficiency.
Imaging Studies
Ultrasound provides excellent visualization of thyroid structure, size, and nodule characteristics. This noninvasive imaging technique helps determine whether nodules are present and evaluates their features. Computed tomography (CT) or magnetic resonance imaging (MRI) may be ordered if airway compression is suspected. Thyroid scintigraphy using radioactive iodine or technetium can assess thyroid function and iodine uptake patterns.
Fine-Needle Aspiration Biopsy
When thyroid nodules are present, fine-needle aspiration (FNA) biopsy may be recommended to evaluate for malignancy. This minimally invasive procedure involves inserting a thin needle into the nodule to obtain cells for microscopic examination.
Treatment Options
Treatment approaches depend on goiter cause, size, symptoms, and thyroid function status.
Iodine Supplementation
For iodine-deficiency goiter, iodine supplementation represents the primary treatment. Iodized salt, dietary sources of iodine, or potassium iodide supplements can restore adequate iodine intake. Most patients show significant improvement within weeks to months of beginning supplementation. Public health initiatives emphasizing iodine fortification have substantially reduced goiter prevalence in many regions.
Thyroid Hormone Replacement
For hypothyroidism-associated goiter, synthetic levothyroxine replaces deficient thyroid hormone and may reduce thyroid volume over time. TSH suppression therapy, using slightly higher doses of levothyroxine to suppress TSH below normal ranges, can help shrink large goiters in some patients with Hashimoto’s thyroiditis.
Antithyroid Medications
For Graves’ disease or hyperthyroid goiter, medications like propylthiouracil (PTU) or methimazole block thyroid hormone production. These medications can reduce gland size as thyroid hormone levels normalize.
Radioactive Iodine Therapy
Radioactive iodine treatment involves ingesting radioactive iodine that concentrates in the thyroid, destroying thyroid tissue. This therapy effectively reduces goiter size in hyperthyroid patients but results in permanent hypothyroidism requiring lifelong hormone replacement.
Surgical Intervention
Thyroidectomy (surgical thyroid removal) may be considered when goiter causes significant compression symptoms affecting breathing or swallowing, contains suspicious nodules, or fails to respond to medical management. Surgery is particularly appropriate for large multinodular goiter with compressive symptoms. Thyroid hormone replacement becomes necessary after thyroidectomy.
When to Seek Medical Attention
Patients should consult healthcare providers if they notice thyroid enlargement, experience difficulty swallowing or breathing, develop hoarseness, or have symptoms suggesting thyroid dysfunction. Persistent neck swelling warrants evaluation to determine cause and appropriate management.
Prevention of Goiter
Prevention strategies focus on maintaining adequate iodine intake through:
- Consuming iodized salt in recommended amounts
- Including seafood and seaweed in the diet
- Eating dairy products and eggs containing iodine
- Using iodine-fortified foods where available
Individuals in iodine-deficient regions or with family history of thyroid disease should maintain particularly vigilant dietary habits. Those taking medications affecting thyroid function should discuss potential goiter risk with their healthcare provider.
Living with Goiter
Most goiter patients can live normal, active lives with appropriate management. Regular follow-up appointments monitor thyroid function and gland size. Maintaining compliance with prescribed medications ensures optimal outcomes. Patients should report new or worsening symptoms promptly to their healthcare team.
Frequently Asked Questions
Q: Can goiter resolve on its own?
A: Mild iodine-deficiency goiter may improve with increased iodine intake. However, established goiter typically requires medical intervention for resolution. Autoimmune goiter rarely resolves without treatment.
Q: Is goiter hereditary?
A: While genetic predisposition exists for autoimmune thyroid diseases causing goiter, environmental factors like iodine deficiency play equally important roles. Family history increases risk but does not guarantee development.
Q: Does goiter affect fertility?
A: Untreated thyroid dysfunction from goiter-causing conditions may impair fertility. However, with appropriate treatment restoring normal thyroid function, fertility typically normalizes.
Q: Can children develop goiter?
A: Yes, children can develop goiter, particularly in iodine-deficient regions. Childhood goiter can affect growth and development, making early diagnosis and treatment important.
Q: Is goiter surgery dangerous?
A: Thyroid surgery is generally safe when performed by experienced surgeons. Potential complications include voice changes from recurrent laryngeal nerve injury and hypoparathyroidism, but these are uncommon.
References
- Hashimoto’s Thyroiditis: Celebrating the Centennial Through Historic Specimens, Evolving Principles, and Unmet Needs — National Institutes of Health/PubMed Central. 2012. https://pmc.ncbi.nlm.nih.gov/articles/PMC3569966/
- Iodine Deficiency Disorders: Classification, Etiology, and Public Health Significance — World Health Organization. 2024. https://www.who.int/teams/nutrition-physical-activity/micronutrients/iodine-deficiency-disorders
- Thyroid Disease and Pregnancy — American Thyroid Association. 2024. https://www.thyroid.org/pregnancy/
- Thyroid Nodules and Goiter — American Academy of Family Physicians. 2023. https://www.aafp.org/afp/2003/0415/p1565.html
Similar Articles






Read full bio of medha deb