Hyperkeratosis Lenticularis Perstans (Flegel Disease) Pathology
Comprehensive pathology overview of Flegel disease: rare keratinization disorder with distinctive hyperkeratotic papules on lower extremities.
 Pathology")
What is hyperkeratosis lenticularis perstans?
Hyperkeratosis lenticularis perstans (HLP), also known as Flegel disease, represents a rare, heritable disorder of keratinization first described by Heinrich Flegel in 1958. This condition manifests as small, red-brown, hyperkeratotic papules primarily affecting the dorsal surfaces of the feet and lower legs. Although initially considered a variant of Kyrle disease, its unique clinical and pathological profile distinguishes it as a separate entity.
The disease typically emerges in adulthood, often in the fourth to sixth decade of life, with a slight predominance in females. Lesions are symmetrically distributed and persist chronically without spontaneous resolution. While benign, HLP causes significant cosmetic distress, prompting patients to seek treatment. Recent genetic studies have identified mutations in the SPTLC1 gene, encoding a subunit of serine palmitoyltransferase, disrupting sphingolipid biosynthesis—a key pathway in epidermal barrier function.
Clinical features
Characteristic lesions of HLP are 1–5 mm red-brown papules topped with adherent, irregular horny scales resembling “corn flakes.” These appear predominantly on the dorsa of feet and lower legs but may extend to thighs, arms, trunk, palms, or rarely mucosal surfaces.
- Symmetric distribution on acral sites
- Asymptomatic or mild pruritus/burning
- Scale removal reveals bright red base with pinpoint bleeding
- Chronic, non-resolving course
- Possible association with endocrinopathies (diabetes, hyperthyroidism)
Family history supports autosomal dominant inheritance with incomplete penetrance. The condition remains stable without malignant potential, though progression to proximal sites occurs over years.
Dermoscopy
Dermoscopy aids non-invasive diagnosis, revealing central brown structureless areas (melanophages, pigment incontinence) surrounded by peripheral scaling, grayish zones (lichenoid infiltrate), brownish reticular patterns, and lacunae-like structures (ectatic dermal vessels). Superficial whitish scaling corresponds to hyper/parakeratosis. Limited reports (fewer than five cases) confirm these patterns’ diagnostic utility, reducing biopsy needs.
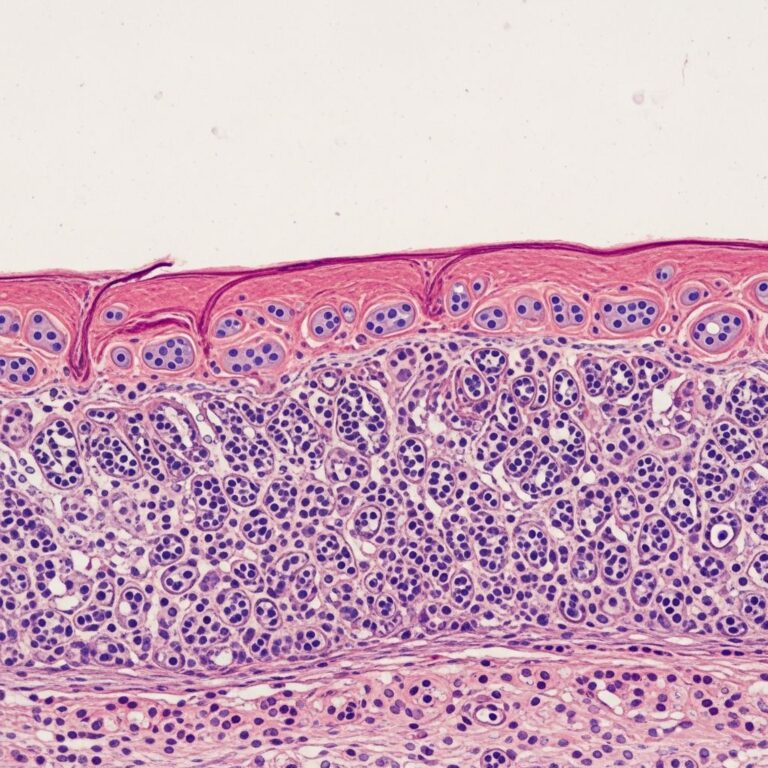
Histopathology
Skin biopsy confirms diagnosis through hallmark features centered on discrete keratin layer abnormalities.
| Key Microscopic Features | Description |
|---|---|
| Stratum corneum | Abrupt compact lamellar hyperkeratosis with focal parakeratosis; peripheral basket-weave orthokeratosis |
| Epidermis | Atrophic/thinned stratum Malpighii; absent/reduced granular layer; irregular acanthosis; basal vacuolation |
| Interface | Lichenoid lymphocytic infiltrate; occasional necrotic keratinocytes/colloid bodies; pigment incontinence |
| Dermis | Band-like chronic inflammation; papillary edema; melanophages |
Immunohistochemistry shows CD3+ T-lymphocytes predominant, with CD4+ > CD8+ ratio. Electron microscopy reveals absent/abnormal Odland bodies (lamellar granules), explaining defective keratinization. No dysplasia or malignancy noted.
Pathogenesis
The precise mechanism remains unclear, but genetic insights illuminate pathophysiology. SPTLC1 mutations reduce serine palmitoyltransferase activity, impairing sphingolipid production essential for barrier integrity and desquamation. This leads to retained corneocytes forming hyperkeratotic plugs.
Secondary factors include:
- Lichenoid interface reaction with cytokine-mediated epidermal damage
- Altered keratinocyte differentiation
- Possible endocrinologic triggers (e.g., diabetes-associated)
Unlike acquired perforating disorders, HLP lacks transepidermal elimination channels.
Differential diagnosis
| Condition | Distinguishing Features |
|---|---|
| Kyrle disease | Larger umbilicated plugs; follicular involvement; diabetes association; less lichenoid infiltrate |
| Porokeratosis | Cornoid lamella; annular lesions |
| Psoriasis | Uniform parakeratosis; Munro microabscesses; regular acanthosis |
| Lichen planus | Wedge-shaped hypergranulosis; Civatte bodies; no focal hyperkeratosis |
| Actinic keratosis | Disordered atypia; solar elastosis |
The abrupt transition from compact to basket-weave hyperkeratosis uniquely favors HLP.
Treatment
No curative therapy exists; management targets symptom relief and cosmesis. Responses vary widely.
- Topical retinoids (tretinoin 0.05%): Promote desquamation; marked improvement in 6–8 weeks
- Topical corticosteroids (betamethasone dipropionate/valerate): Reduce inflammation; good response reported
- Keratolytics/Emollients (urea, salicylic acid): Soften scales
- 5-Fluorouracil (topical): Superior to vitamin D analogs; variable success
- Other: Calcipotriol, PUVA phototherapy, oral retinoids (refractory cases)
Patient education emphasizes chronicity and benign nature. Aggressive therapies often declined due to modest efficacy. Future sphingolipid-modulating agents hold promise.
Frequently Asked Questions (FAQs)
Is Flegel disease contagious?
No, hyperkeratosis lenticularis perstans is a genetic keratinization disorder, not infectious.
Does Flegel disease cause cancer?
No evidence links HLP to malignancy; lesions are benign.
Can Flegel disease be cured?
No cure exists, but topical therapies control symptoms effectively for many.
Who gets Flegel disease?
Typically adults 40–60 years old; autosomal dominant inheritance with late onset.
Is biopsy always needed for diagnosis?
Clinical + dermoscopy often sufficient; biopsy confirms in atypical cases.
References
- Hyperkeratosis Lenticularis Perstans (Flegel Disease) — PMC. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11927986/
- Hyperkeratosis lenticularis perstans (Flegel’s disease) – successful treatment — Wiley Online Library. 2008-11-01. https://onlinelibrary.wiley.com/doi/10.1111/j.1365-4632.2008.03958.x
- Hyperkeratosis Lenticularis Perstans (Flegel Disease) — DermNet NZ. 2023. https://dermnetnz.org/topics/hyperkeratosis-lenticularis-perstans
- Hyperkeratosis lenticularis perstans (Flegel disease) — Pathological Society. 2020-03. https://www.pathsoc.org/_userfiles/pages/files/education/mpdhp_mar_2020_short_case.pdf
- Hyperkeratosis lenticularis perstans aka Flegel’s disease — Medizin Online. 2023. https://medizinonline.com/en/hyperkeratosis-lenticularis-perstans-aka-flegels-disease/
Similar Articles






Read full bio of medha deb