Hysterectomy Guide: What To Expect, Recovery & Risks
Comprehensive overview of hysterectomy surgery: types, reasons, procedures, recovery, and life after uterus removal for informed decisions.

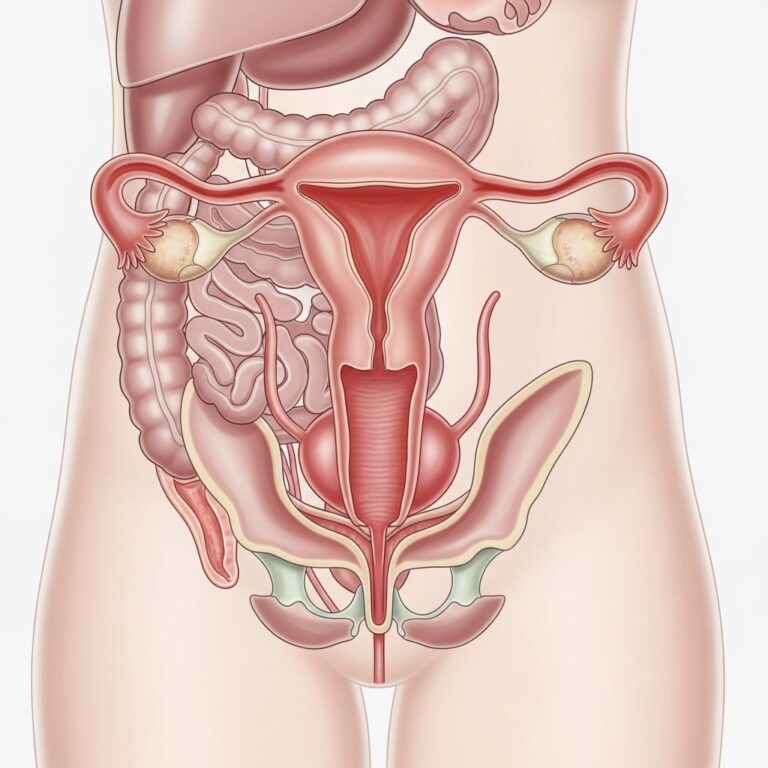
A hysterectomy involves the surgical removal of the uterus, a procedure often recommended for various gynecological conditions that significantly impact quality of life. This surgery ends menstruation and the ability to conceive, marking a pivotal health decision for many women.
Understanding When Hysterectomy Becomes Necessary
Medical professionals recommend hysterectomy when non-surgical treatments fail to alleviate persistent uterine issues. Common indications include benign tumors known as uterine fibroids, which cause heavy bleeding and pelvic discomfort; endometriosis, where uterine tissue grows outside the organ leading to chronic pain; and uterine prolapse, in which the uterus descends into the vaginal canal due to weakened support structures.
Cancerous conditions, such as uterine or cervical cancer, may necessitate more extensive removal, while abnormal bleeding unresponsive to medications or procedures like endometrial ablation also prompts this surgery. In cases of severe pelvic inflammatory disease or chronic pain syndromes, hysterectomy provides definitive relief.
Different Types of Hysterectomy Procedures
Hysterectomies vary based on the extent of tissue removal and surgical access method, tailored to the patient’s anatomy, condition severity, and surgeon expertise.
- Total hysterectomy: Removes the entire uterus and cervix, standard for most non-cancerous cases.
- Supracervical or subtotal hysterectomy: Excises only the upper uterus, preserving the cervix to potentially reduce recovery time and maintain pelvic support.
- Radical hysterectomy: Involves uterus, cervix, upper vagina, and surrounding tissues, primarily for cancer treatment, often including lymph node dissection.
Additional removals may include ovaries (oophorectomy) and fallopian tubes (salpingectomy), influencing hormone production and menopause onset.
Surgical Approaches: From Traditional to Advanced
Surgeons select approaches balancing invasiveness, recovery speed, and complication risks. Abdominal hysterectomy uses a large incision for direct access, suitable for large fibroids or adhesions.
Minimally invasive options predominate today:
| Approach | Description | Incisions | Recovery Time |
|---|---|---|---|
| Abdominal | Uterus removed via lower abdomen | One large (6-8 inches) | 4-6 weeks |
| Vaginal | Through vaginal canal, no abdominal cut | None external | 2-4 weeks |
| Laparoscopic | Small ports for camera/tools | 3-5 small | 1-3 weeks |
| Robot-assisted | Robotic precision via laparoscopy | 3-5 small | 1-3 weeks |
Vaginal suits smaller uteri without extensive disease; laparoscopic and robotic enhance visualization and precision, reducing blood loss and hospital stays.
Preparing for Your Hysterectomy Surgery
Preparation optimizes outcomes. Consultations assess overall health, discussing medical history, medications, and fertility goals. Preoperative tests include blood work, imaging, and cardiac evaluations if needed.
Lifestyle adjustments: Quit smoking to aid healing, maintain nutrition, and practice pelvic floor exercises. Fasting protocols and bowel prep clear the surgical field. Emotional support via counseling addresses anxiety over body changes.
Plan logistics: Arrange home help, as initial recovery limits driving and lifting.
Inside the Operating Room: What Happens During Surgery
A typical abdominal hysterectomy follows structured steps to minimize risks like ureter injury. After anesthesia induction and laparotomy, surgeons ligate the round ligament, ovarian ligament, and Fallopian tubes if indicated. Bladder mobilization exposes key vessels.
Critical phases clamp uterine arteries, cardinal and sacrouterine ligaments sequentially, pushing ureters laterally for safety. Vaginal incision allows uterus extraction, followed by cuff closure, hemostasis, and layered abdominal repair.
Related Stories



Minimally invasive variants use ports for similar dissections, morcellating the uterus for removal. Procedures last 1-3 hours.
Immediate Post-Operative Care and Hospital Stay
Patients awaken in recovery monitoring vital signs, pain, and bleeding. Hospital stays range 1-5 days: same-day discharge for vaginal/laparoscopic, longer for abdominal.
Pain management combines opioids, NSAIDs, and nerve blocks. Catheters drain urine 1-2 days; early ambulation prevents clots. Clear liquids progress to solids.
Recovery Timeline at Home
Full recovery spans 2-8 weeks. Week 1: Rest, light walking, wound care. Avoid baths, intercourse, tampons 6 weeks.
- Weeks 1-2: Fatigue common; manage constipation with stool softeners.
- Weeks 3-4: Resume light activities; fatigue eases.
- Weeks 5-6: Return to work if non-physical; gradual exercise.
Follow-up checks healing at 2 and 6 weeks.
Potential Risks and Complications
Though safe (mortality <0.1%), risks include infection, bleeding, bowel/bladder injury (1-2%), and thromboembolism. Long-term: Vaginal cuff dehiscence (rare), fistula, or prolapse. Hormone loss if ovaries removed accelerates menopause.
Navigating Life After Hysterectomy
No periods or pregnancy post-surgery; libido often preserved. Menopause symptoms if ovaries gone: hot flashes, mood changes—managed by hormone therapy or alternatives.
Pelvic support may weaken; Kegels strengthen muscles. Sexual function improves sans pain from prior conditions. Bone health monitoring essential.
Alternatives to Consider Before Surgery
Explore medications (e.g., GnRH agonists for fibroids), uterine artery embolization, myomectomy, or endometrial ablation. Hysterectomy is last resort.
Frequently Asked Questions (FAQs)
Will I enter menopause immediately?
Only if ovaries removed; otherwise, natural transition later.
How long until driving?
1-2 weeks post-minimally invasive; longer for abdominal.
Does it affect sexual pleasure?
Typically no; many report improvement.
Can it treat cancer?
Yes, especially radical type.
Weight gain common?
Not directly; lifestyle factors influence.
Empowering Decisions: Talking to Your Doctor
Discuss pros/cons, personal risks, and second opinions. Shared decision-making ensures alignment with values.
References
- Basic Standard Procedure of Abdominal Hysterectomy: Part 1 — PMC/NCBI. 2019-05-28. https://pmc.ncbi.nlm.nih.gov/articles/PMC6554021/
- Hysterectomy | Fact Sheets — Yale Medicine. Accessed 2026. https://www.yalemedicine.org/conditions/hysterectomy
- Hysterectomy: Types, Recovery, Pain Management — American Society of Anesthesiologists. Accessed 2026. https://madeforthismoment.asahq.org/preparing-for-surgery/procedures/hysterectomy/
- Hysterectomy | What to Expect | FAQs — IU Health. Accessed 2026. https://iuhealth.org/find-medical-services/hysterectomy
- Hysterectomy — ACOG. Accessed 2026. https://www.acog.org/womens-health/faqs/hysterectomy
- Hysterectomy: Surgery, Types, Side Effects & Recovery — Cleveland Clinic. Accessed 2026. https://my.clevelandclinic.org/health/procedures/hysterectomy
Similar Articles






Read full bio of Sneha Tete