Incontinentia Pigmenti: Symptoms, Causes & Treatment
Understanding incontinentia pigmenti: A comprehensive guide to this rare genetic skin disorder and its management.

Incontinentia Pigmenti: An Overview
Incontinentia pigmenti (IP), also known as Bloch-Sulzberger syndrome or Bloch-Siemens syndrome, is a rare X-linked dominant genetic disorder that affects multiple organ systems, including the skin, hair, teeth, eyes, and central nervous system. This neurocutaneous disorder is characterized by progressive skin pigmentation abnormalities that typically appear in the first weeks of life, accompanied by various systemic manifestations. The condition results from mutations in the IKBKG gene, which plays a crucial role in regulating cellular inflammation and survival pathways.
Genetic Basis and Pathophysiology
The IKBKG Gene Mutation
Incontinentia pigmenti is caused by mutations in the IKBKG gene, located on the X chromosome at position q28. This gene is also known as NEMO (Nuclear Factor κβ Essential Modulator) or IKK-γ (Inhibitor of nuclear factor Kappa-B Kinase, subunit gamma). The gene was identified in 2000 through collaborative research efforts, representing a significant advancement in understanding this rare disorder.
Approximately 60 to 80 percent of affected individuals carry deletions in the IKBKG gene that remove genetic material, resulting in the production of an abnormally small, nonfunctional version of the IKBKG protein. Other individuals with IP have variants that prevent the production of any IKBKG protein altogether. This loss of functional protein disrupts the regulation of the nuclear factor-kappa-B (NF-κB) pathway, making cells abnormally sensitive to signals that trigger programmed cell death (apoptosis).
Molecular Mechanisms
The pathophysiology of incontinentia pigmenti involves several interconnected mechanisms. With the mutated IKBKG gene, endothelial cells and other cells throughout the body over-express chemotactic factors specific for eosinophils, explaining the common occurrence of serum eosinophilia in IP patients. The epidermal skin lesions demonstrate extensive involvement of eosinophils, which combine with other inflammatory factors to create extensive inflammation affecting not only the skin but also endothelial cells.
This inflammatory cascade is believed to lead to vaso-occlusion (blocking of blood vessels), which results in ischemia (reduced blood supply). This ischemic process causes both the retinal and neurologic manifestations of IP. However, the pathophysiology is complex, as there is limited evidence that typical inflammatory pathology in the skin also occurs in the retina, and vaso-occlusion in skin lesions is not consistently documented.
Epidemiology and Inheritance Pattern
Incontinentia pigmenti is a rare genetic disorder with no known ethnic or racial predisposition. The exact prevalence is unknown, as IP is frequently undiagnosed or misdiagnosed. However, because the gene defect occurs on the X chromosome, the condition is most often seen in females. When it occurs in males, it is typically lethal in the fetus, resulting in miscarriage. This X-linked dominant inheritance pattern explains why the vast majority of individuals with IP are female, and when males are affected, they present with more severe manifestations.
Clinical Features and Skin Manifestations
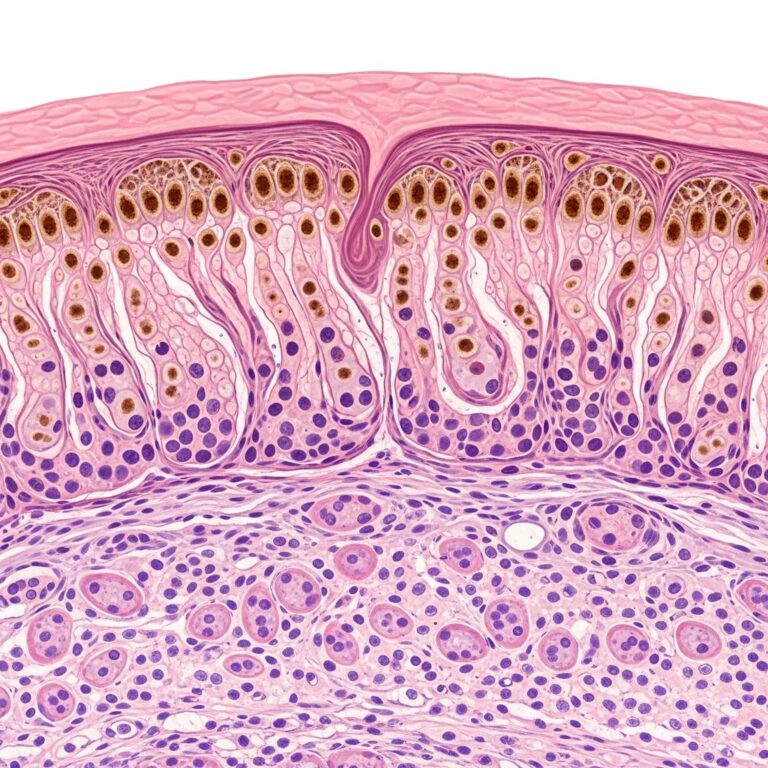
Characteristic Skin Lesions
The most distinctive feature of incontinentia pigmenti is the characteristic skin pigmentation pattern. Most newborns with IP develop discolored skin within the first two weeks of life. The pigmentation involves the trunk and extremities and typically appears as slate-grey, blue, or brown coloration distributed in irregular marbled or wavy lines following Blaschko’s lines.
The skin lesions of incontinentia pigmenti progress through four distinct stages over time:
- Stage 1 (Vesicular/Inflammatory): Blistering and inflammatory lesions appear, often within the first two weeks of life. These lesions may be mistaken for other conditions such as herpes, chickenpox, or other viral infections.
- Stage 2 (Verrucous): Wart-like bumps develop, typically appearing within weeks to months after the vesicular stage.
- Stage 3 (Hyperpigmented): The lesions become increasingly pigmented, developing the characteristic slate-grey, blue, or brown coloration in a marbled or wavy pattern.
- Stage 4 (Hypopigmented/Atrophic): Progressive loss of pigmentation and skin atrophy occur, often by adolescence or adulthood, with possible scarring.
Disease Course and Prognosis
A significant characteristic of incontinentia pigmenti is that the skin abnormalities often resolve spontaneously by adolescence or early adulthood without specific treatment. Stage 1 and 2 lesions may recur with routine febrile illness well into adulthood. However, the complete resolution of skin manifestations does not indicate resolution of systemic complications, which may persist or progress.
Extracutaneous Manifestations
Ocular Abnormalities
Incontinentia pigmenti commonly includes eye abnormalities, most occurring in the retina. The retinal findings stem from vascular occlusion and include:
- Neovascularization (abnormal new blood vessel formation)
- Retinal hemorrhages
- Absence of foveal pit
- Exudative and tractional retinal detachments
- Diffuse mottled hypopigmentation in the retina
- Peripheral avascular areas (non-perfused retinal regions)
Additional non-retinal ocular manifestations include cataracts, uveitis, strabismus (occurring in approximately 18% of patients), conjunctival pigmentation, optic atrophy (in 5% of patients), and nystagmus. If untreated, ocular IP can result in phthisis bulbi (shrinkage and degeneration of the eye). Importantly, retinal detachments nearly always occur within six years of age and are relatively rare in older patients.
Dental Abnormalities
Pathologic changes in the teeth are common in incontinentia pigmenti. Affected individuals may experience delayed tooth eruption, abnormal tooth development, missing teeth, or structural anomalies in dental enamel. Dental complications may require specialist evaluation and management.
Hair Loss
Hair abnormalities are frequent in IP, with 60 to 80 percent of affected individuals experiencing some degree of alopecia (hair loss) on the scalp and other parts of the body. Hair loss can be patchy or more widespread and may vary in severity among affected individuals.
Neurological Manifestations
Pathologic changes in the central nervous system are common in incontinentia pigmenti. Neurological manifestations may include:
- Seizures (in some affected individuals)
- Muscle spasms
- Mild to moderate paralysis
- Developmental delays
- Intellectual disabilities
- Cerebral and cerebellar atrophy
These neurological sequelae are believed to result from vaso-occlusive ischemia in the central nervous system, similar to the mechanisms affecting the retina. The degree of neurological involvement varies significantly among affected individuals.
Other Features
Additional features of incontinentia pigmenti may include skeletal abnormalities, reduced sweating (leading to heat intolerance and risk of dangerous overheating), and increased risk of certain malignancies. Individuals with IP require careful monitoring for cutaneous squamous cell carcinoma.
Diagnosis
Clinical Evaluation
Diagnosis of incontinentia pigmenti is based on a comprehensive clinical evaluation including systemic and ocular examination. The characteristic pattern of skin lesions in a newborn or young infant, combined with the presence of systemic manifestations, should raise suspicion for IP. Early recognition is important because timely intervention can prevent serious complications, particularly retinal detachment.
Genetic Testing
Genetic testing is the definitive diagnostic method for confirming incontinentia pigmenti. DNA sequencing to identify mutations in the IKBKG gene provides confirmation of the diagnosis and enables genetic counseling for affected families. Genetic testing can also identify carrier status in family members.
Imaging Studies
Brain imaging, typically MRI (magnetic resonance imaging), should be obtained to investigate the occlusive consequences of IP in the brain. EEG (electroencephalography) should be performed if seizures are present or suspected. Regular ophthalmologic imaging, including retinal examination and imaging, is essential to detect and monitor retinal abnormalities.
Treatment and Management
General Treatment Approach
Because incontinentia pigmenti is a multi-system condition, comprehensive multidisciplinary care is essential. Management should involve coordination among:
- Dermatologists
- Geneticists
- Ophthalmologists and retina specialists
- Neurologists
- Dental specialists
- Developmental specialists and pediatricians
Dermatologic Management
There are no directed treatments for the characteristic skin lesions of IP. Topical steroids are not effective. However, proper skin care is important to prevent complications:
- Keep skin lesions clean and dry
- Minimize irritation to avoid secondary bacterial infection
- Protect lesions from trauma and environmental damage
- Monitor for signs of infection and treat promptly if they develop
- Provide regular monitoring and evaluation for cutaneous squamous cell carcinoma
Since the skin abnormalities often resolve spontaneously by adolescence or adulthood, reassurance to families about the likely favorable skin prognosis is important, even though systemic complications may persist.
Ophthalmologic Management
Preventing vision loss is a critical component of IP management. Treatment options for ocular manifestations include:
- Regular retinal examination: Frequent monitoring by a retina specialist is essential to detect retinal changes early
- Laser photocoagulation: Used to treat retinal neovascularization that predisposes to retinal detachment
- Cryotherapy: May be used in conjunction with or instead of laser treatment for retinal abnormalities
- Surgical intervention: Required in cases of established retinal detachment or significant vitreous hemorrhage
- Corrective lenses: For refractive errors and diminished vision
- Medication: Various medications may be used to manage associated conditions like uveitis
Neurological Management
Neurological symptoms should be managed by a neurologist and may include:
- Seizure management: Anticonvulsant medications to control seizures if present
- Management of muscle spasms and paralysis: Various medications and/or medical devices as appropriate
- Developmental support: Early intervention therapy and developmental services for children with developmental delays
- Educational support: School assistance and accommodations for children with intellectual disabilities
Dental and Other Specialist Care
Dental specialists should manage dental abnormalities, which may include restorative work or orthodontic intervention. Additional specialist consultations should be obtained as needed for specific complications.
Management of Heat Intolerance
Because reduced sweating can lead to heat intolerance and dangerous overheating, affected individuals should:
- Use cool baths and showers
- Apply ice packs as needed
- Seek shade and avoid prolonged sun exposure
- Wear appropriate lightweight clothing
- Monitor body temperature carefully during febrile illnesses
Genetic Therapies and Future Directions
Genetic therapies are not currently available for incontinentia pigmenti. However, research into potential gene therapy approaches is ongoing. Current management remains focused on symptomatic treatment and prevention of complications through multidisciplinary care.
Frequently Asked Questions
Q: Is there a cure for incontinentia pigmenti?
A: There is currently no cure for incontinentia pigmenti. However, symptoms and complications can be managed through multidisciplinary medical and surgical intervention. Many skin manifestations resolve spontaneously by adulthood.
Q: Will my child’s skin lesions persist throughout life?
A: No. The characteristic skin abnormalities of IP typically disappear by adolescence or early adulthood in many individuals. However, other systemic complications may require ongoing management.
Q: What is the inheritance pattern of incontinentia pigmenti?
A: IP is inherited in an X-linked dominant pattern. It usually affects females, as the condition is typically lethal in affected males. Carrier mothers have a 50% chance of passing the mutation to each child.
Q: How is incontinentia pigmenti diagnosed?
A: Diagnosis is based on clinical examination of the characteristic skin lesions and systemic manifestations, combined with genetic testing to confirm mutations in the IKBKG gene.
Q: What is the most serious complication of incontinentia pigmenti?
A: Retinal detachment is one of the most serious complications, particularly when it occurs in young children. Regular ophthalmologic monitoring and early intervention with laser photocoagulation or surgery can prevent vision loss.
Q: Can incontinentia pigmenti be prevented?
A: Since IP is a genetic disorder, it cannot be prevented. However, genetic counseling can help families understand inheritance patterns and reproductive risks.
References
- Incontinentia Pigmenti — EyeWiki (American Academy of Ophthalmology). 2024. https://eyewiki.org/Incontinentia_Pigmenti
- Incontinentia pigmenti — Genetics — MedlinePlus, National Library of Medicine. 2024. https://medlineplus.gov/genetics/condition/incontinentia-pigmenti/
- Incontinentia Pigmenti: Symptoms & Diagnosis — NFED (National Foundation for Ectodermal Dysplasias). 2024. https://nfed.org/learn/types/incontinentia-pigmenti/
- Incontinentia Pigmenti — Symptoms, Causes, Treatment — NORD (National Organization for Rare Disorders). 2024. https://rarediseases.org/rare-diseases/incontinentia-pigmenti/
- Incontinentia Pigmenti (Bloch-Sulzberger Syndrome) — NCBI Bookshelf, National Center for Biotechnology Information. 2024. https://www.ncbi.nlm.nih.gov/books/NBK578194/
- Incontinentia Pigmenti — UF Health (University of Florida Health). 2024. https://ufhealth.org/conditions-and-treatments/incontinentia-pigmenti
- Incontinentia Pigmenti (Bloch-Sulzberger Syndrome) — BrainFacts.org, Society for Neuroscience. 2024. https://www.brainfacts.org/diseases-and-disorders/neurological-disorders-az/diseases-a-to-z-from-ninds/incontinentia-pigmenti
Similar Articles






Read full bio of Sneha Tete