Keratoacanthoma: Clinical Features and Visual Guide
Visual and clinical guide to keratoacanthoma: identification, diagnosis, and management.

Introduction to Keratoacanthoma
Keratoacanthoma (KA) is a common, rapidly growing, locally destructive skin tumor that presents significant clinical and diagnostic challenges. This condition typically develops on sun-exposed areas and shares many features with well-differentiated squamous cell carcinoma (SCC), making proper identification essential. While keratoacanthomas may regress spontaneously with scarring, their clinical course is often unpredictable, and they may be indistinguishable from malignant lesions. Many clinicians and pathologists now prefer the term SCC, KA-type and recommend surgical excision to ensure accurate diagnosis and appropriate management.
Demographics and Epidemiology
Keratoacanthomas are relatively common skin growths that can affect individuals across various age groups and backgrounds. These lesions typically present as solitary lesions on sun-exposed skin, particularly on the face and upper limbs. While keratoacanthomas are significantly less common in patients with skin of color, the clinical features remain consistent across all skin types. The condition shows a predilection for older adults with extensive sun exposure history, though it can develop at any age. Both men and women are affected, though some studies suggest a slight male predominance.
Clinical Features and Presentation
Keratoacanthomas typically present as a solitary, rapidly growing nodule on sun-exposed skin. The characteristic appearance includes sharply demarcated, firm, erythematous or skin-colored lesions with a classic central hyperkeratotic plug and an even shoulder. A distinctive feature is the crater-like appearance visible when the keratotic core is removed, giving the lesion a volcano-like morphology.
Initial Presentation
Lesions begin as small, round pink or skin-colored papules that undergo rapid growth to dome-shaped nodules within weeks. Patients often initially mistake keratoacanthomas for pimples or boils, but the rapid growth pattern distinguishes them from common skin lesions. Within one to two months, these growths typically expand to approximately one inch (2.5 centimeters) wide, though some may grow twice as large.
Characteristic Morphology
The defining characteristics of keratoacanthoma include:
- Round, firm, usually flesh-colored dome-shaped appearance
- Central crater that is scaly or crusted, often containing keratin or dead skin cells
- Well-defined borders with an even shoulder surrounding the central plug
- Rapid growth phase followed by stabilization
- Occasional itching or pain reported by patients
Location and Sun Exposure Patterns
Keratoacanthomas predominantly occur on sun-exposed, hair-bearing areas of the body. The most common locations include the face, head, neck, and dorsum of extremities. Other frequently affected areas encompass the backs of the hands, forearms, and sometimes the legs. Lesions on the trunk are uncommon, as these areas receive less cumulative sun exposure. The typical origin point is often within a hair follicle, particularly in areas with high-density hair-bearing skin.
Clinical Features Across Skin Types
While keratoacanthomas are much less common in patients with skin of color, the clinical features remain essentially consistent across all skin types. Darker-skinned individuals may present with similar dome-shaped morphology and central hyperkeratotic plugs, though the erythema may be less apparent. The same rapid growth pattern, crater-like appearance, and predilection for sun-exposed areas characterize lesions in all populations. Recognition of these features across diverse skin types is crucial for timely diagnosis and appropriate management.
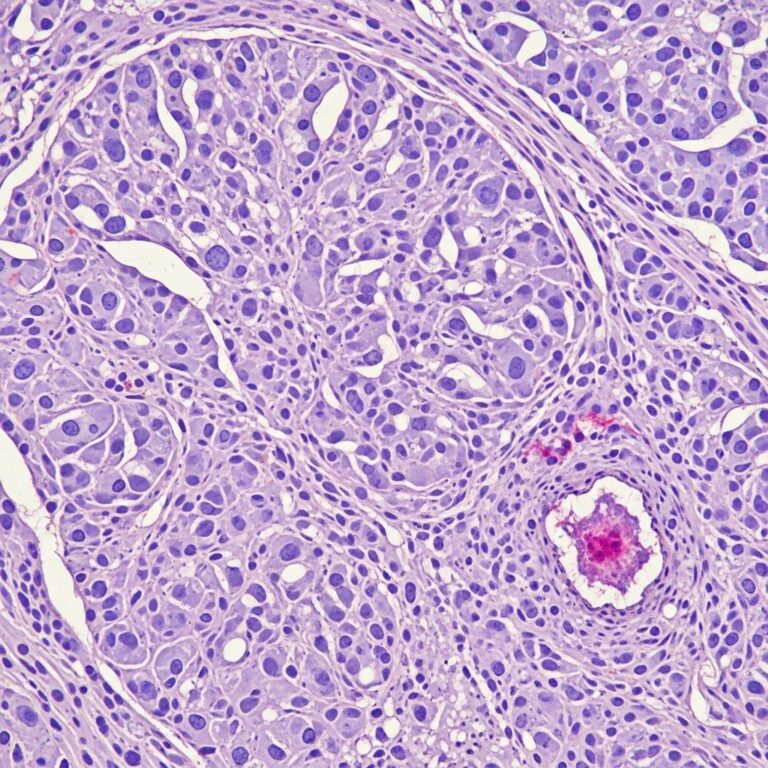
Histopathological Features and Diagnosis
Keratoacanthoma is diagnosed on the basis of a typical history, clinical signs, and histopathology. The classic keratoacanthoma has a crateriform appearance when viewed histologically at low power. Higher power examination reveals enlarged atypical keratinocytes with eosinophilic cytoplasm that do not extend beyond the level of the sweat glands.
Histological Characteristics
The histopathological examination of keratoacanthoma demonstrates:
- Multilobular exophytic or endophytic cyst-like invagination of the epidermis
- Central horn plug of keratin surrounded by lip-like peripheral borders
- Intraepidermal neutrophilic abscesses and horn pearls
- Enlarged and atypical keratinocytes with eosinophilic cytoplasm
- Lesion confined to the dermis without extension beyond sweat gland level
Diagnostic Limitations
Partial or shave biopsy samples are not recommended, as they may fail to demonstrate the characteristic histological features necessary for accurate diagnosis. Some otherwise typical keratoacanthomas show squamous cells in a peripheral zone with atypical mitotic figures, hyperchromatic nuclei, and penetration into surrounding tissue. Such lesions are often reported as SCC, KA-type to reflect uncertainty about their true nature. Unfortunately, dermoscopy cannot reliably discriminate keratoacanthoma from squamous cell carcinoma, necessitating histopathological examination for definitive diagnosis.
Clinical Course and Natural History
Keratoacanthoma is characterized by initial rapid growth followed by a period of variable tumor stability and spontaneous regression. The condition progresses through three distinct stages:
| Stage | Duration | Characteristics |
|---|---|---|
| Proliferation | 6-8 weeks | Rapid growth to peak size; lesion expands quickly |
| Maturation | Several weeks to months | Maintains crateriform appearance; tumor stabilizes |
| Involution | Variable duration | Spontaneous regression into atrophic scar |
While spontaneous regression may occur, keratoacanthomas may spontaneously disappear within several months, often leaving a scar. However, because of the unpredictable clinical course and the difficulty distinguishing keratoacanthoma from malignant squamous cell carcinoma clinically, many clinicians prefer to recommend surgical excision for definitive diagnosis.
Complications Associated with Keratoacanthoma
Several complications can arise from keratoacanthoma, including:
- Permanent scarring from spontaneous regression
- Local tissue destruction due to the tumor’s growth
- Infection of the central crater
- Bleeding or ulceration of the lesion
- Psychological impact related to cosmetically visible lesions
- Diagnostic uncertainty and potential mismanagement
Differential Diagnosis
Keratoacanthomas must be distinguished from well-differentiated squamous cell carcinoma and other conditions with similar presentation. Differential diagnoses include:
- Well-differentiated squamous cell carcinoma (SCC)
- Basal cell carcinoma
- Amelanotic melanoma
- Sebaceous cyst or epidermoid cyst
- Pyogenic granuloma
- Bowen disease
- Wart or common verruca
The clinical and histopathological overlap between keratoacanthoma and well-differentiated squamous cell carcinoma remains a significant diagnostic challenge. Lesions that progress and metastasize have probably been squamous cell carcinoma, KA-type all along, underscoring the importance of complete excision and thorough histological examination.
Treatment Approaches
Management options for keratoacanthoma vary based on lesion characteristics, location, and clinical presentation:
Surgical Excision
Complete surgical excision remains the preferred treatment modality, providing both therapeutic benefit and tissue for definitive histopathological diagnosis. This approach ensures complete removal and allows differentiation from malignant lesions.
Cryotherapy
Small keratoacanthomas can occasionally be treated by freezing with liquid nitrogen (cryotherapy), a less invasive option suitable for selected cases with limited size.
Topical and Intralesional Chemotherapy
Keratoacanthoma may be treated with topical or intralesional (via injection) chemotherapy, offering alternatives to surgical intervention in specific clinical scenarios.
Syndrome-Associated Keratoacanthomas
Certain rare genetic conditions can cause multiple keratoacanthomas to develop simultaneously. These hereditary syndromes include:
Ferguson-Smith Syndrome
This autosomal dominant condition represents the most common type of multiple keratoacanthoma and can cause as many as 100 keratoacanthomas at one time. It is a genetic condition that may start as early as age 8, presenting significant management challenges as doctors cannot remove all lesions surgically.
Other Syndrome Associations
Additional syndromes associated with keratoacanthoma include:
- Muir-Torre syndrome (autosomal dominant)
- Xeroderma pigmentosum (autosomal recessive)
- Incontinentia pigmenti (X-linked dominant)
- Witten-Zak syndrome (autosomal dominant)
- Generalized eruptive keratoacanthoma of Grzybowski
Risk Factors and Etiology
Multiple etiologies have been suggested for keratoacanthoma development, including ultraviolet (UV) radiation exposure, chemical carcinogen exposure, immunosuppression, and genetic predisposition. BRAF inhibitor use has emerged as a potential risk factor. Genetic mutations involving p53 or H-Ras may contribute to lesion formation. Viral exposure, including human papillomavirus (HPV), and recent trauma or surgery to the location have also been implicated in keratoacanthoma development.
Patient Management and Follow-up
For patients with keratoacanthoma, regular skin examination and appropriate preventive measures are essential:
Self-Care Recommendations
- Check your skin regularly for any new lumps or bumps
- Avoid getting sunburnt through consistent sun protection
- Use high-factor sunscreen (minimum SPF 30) with broad-spectrum protection against both UVA and UVB radiation
- Apply sunscreen to exposed areas including face, hands, neck, and other sun-exposed regions
- Seek regular dermatological evaluation
Follow-up Care
Patients have an increased incidence of other sun-related skin cancers and should be advised about sun protection and self-examination. Regular dermatological surveillance is recommended to monitor for recurrent lesions or development of other skin malignancies.
Frequently Asked Questions (FAQs)
Q: Is keratoacanthoma cancerous?
A: Keratoacanthoma is typically benign, but it shares features with squamous cell carcinoma and cannot always be reliably distinguished clinically or dermoscopically. Most clinicians recommend surgical excision for definitive diagnosis to rule out malignancy.
Q: Can keratoacanthoma disappear on its own?
A: Yes, keratoacanthomas may regress spontaneously over several months, but this process typically results in scarring and the clinical course is unpredictable. Surgical removal is often preferred to control the outcome and prevent complications.
Q: How quickly does keratoacanthoma grow?
A: Keratoacanthoma is characterized by rapid initial growth, typically reaching its full size of approximately one inch (2.5 centimeters) within one to two months, though some lesions may grow larger.
Q: Where does keratoacanthoma typically appear?
A: Keratoacanthomas most commonly develop on sun-exposed, hair-bearing areas including the face, head, neck, and backs of the hands and forearms. They rarely appear on the trunk.
Q: Are there preventive measures for keratoacanthoma?
A: While prevention is not always possible, sun protection using SPF 30 or higher broad-spectrum sunscreen on exposed areas and avoiding sunburn may reduce the risk of developing keratoacanthomas and other sun-related skin lesions.
Q: Is keratoacanthoma more common in specific populations?
A: Keratoacanthomas are much less common in patients with skin of color compared to fair-skinned individuals, though they can occur in all populations with similar clinical features.
References
- Keratoacanthoma — DermNet New Zealand. Accessed January 2026. https://dermnetnz.org/topics/keratoacanthoma
- Keratoacanthoma — StatPearls, National Center for Biotechnology Information (NCBI). Updated 2024. https://www.ncbi.nlm.nih.gov/books/NBK499931/
- What is Keratoacanthoma? Causes, Symptoms, Prevention, Treatment — WebMD. Accessed January 2026. https://www.webmd.com/melanoma-skin-cancer/keratoacanthoma-skin-tumor
- Keratoacanthoma — Merck Manuals. Accessed January 2026. https://www.merckmanuals.com/home/skin-disorders/skin-cancers/keratoacanthomas
- Keratoacanthoma — BAD Patient Hub, Skin Health Info, British Association of Dermatologists. Accessed January 2026. https://www.skinhealthinfo.org.uk/condition/keratoacanthoma/
- Keratoacanthoma — Primary Care Dermatology Society (PCDS). Accessed January 2026. https://www.pcds.org.uk/clinical-guidance/keratoacanthoma
- Keratoacanthoma: Symptoms, Causes & Treatment — Cleveland Clinic. Accessed January 2026. https://my.clevelandclinic.org/health/diseases/keratoacanthoma
Similar Articles






Read full bio of medha deb