Lipoma: Causes, Diagnosis, Treatment And Key Facts
Benign fatty tumours: causes, diagnosis, and safe removal options for common subcutaneous lumps.

A
lipoma
is a very common benign, slow-growing tumour composed of mature fat cells (adipocytes), typically developing in the subcutaneous tissue beneath the skin. These soft, rubbery lumps are usually painless and harmless, though they can occasionally cause discomfort if large or pressing on nearby structures.What is a lipoma?
Lipomas represent overgrowths of well-differentiated adipocytes forming a benign neoplasm. They are the most frequent mesenchymal soft tissue tumour, affecting approximately 1 in 1,000 individuals. While predominantly subcutaneous, rare variants extend deeper into fascial planes, intramuscularly, or even internally (e.g., gastrointestinal tract, mediastinum). Single lipomas predominate, but 5-10% of cases involve multiple lesions, often linked to genetic syndromes.
Histologically, lipomas consist of mature adipose tissue lobules encased in a thin fibrous capsule, with minimal vascularity and no cytological atypia. Genetic rearrangements, such as 12q13-15 translocations involving MDM2 or HMGA2 genes, occur in about 50-70% of cases but are not routinely tested.
Who gets lipomas?
Lipomas typically arise in adults aged 40-60 years, with a slight male predominance. They are uncommon in children unless syndromic. No strong racial or ethnic predisposition exists, and clinical presentation remains consistent across Fitzpatrick skin types.
Risk factors include:
- Family history (e.g., familial multiple lipomatosis)
- Obesity (mild association)
- Trauma (controversial; may trigger growth in predisposed sites)
- Genetic syndromes (see below)
What causes lipomas?
The precise aetiology remains unclear, but lipomas arise from multipotent adipose stem cells undergoing monoclonal expansion. Cytogenetic studies reveal consistent abnormalities:
- Conventional lipomas: t(12q13-15) in 33-65%
- Atypical lipomas: Ring chromosomes or MDM2 amplification
- Variants: Specific translocations (e.g., 6p21-23 in lipomas of forearm; 13q in hibernomas)
Environmental triggers like trauma or adipose injury may promote proliferation in genetically susceptible individuals. No modifiable lifestyle factors are definitively proven.
What are the clinical features of lipoma?
Lipomas manifest as solitary or multiple, painless, soft-to-firm, lobulated subcutaneous nodules measuring 1-10+ cm. Key characteristics include:
- Site: Trunk (50%), proximal extremities (shoulders, arms, thighs), neck, forehead. Rare in distal limbs, palms, soles.
- Appearance: Skin overlying is normal, mobile (slips freely). Lumps feel doughy, compressible, non-tender unless inflamed or vascular.
- Growth: Slow over months-years; stable size common.
- Symptoms: Asymptomatic usually; pain if compressing nerves/vessels (e.g., intramuscular), rapid growth, or angiolipoma variant.
Clinical features do not vary by skin tone. On palpation, lobulation is evident; dermoscopy shows uniform yellow-white ovoid structures.
Multiple lipomas
Approximately 5-10% of patients develop multiple lipomas (>3), warranting evaluation for syndromes:
| Syndrome | Features | Associations |
|---|---|---|
| Familial multiple lipomatosis | 20-50 symmetrical lipomas on extremities/trunk | Autosomal dominant |
| Proteus syndrome | Asymmetric overgrowth + lipomas | AKT1 mutation; scoliosis, seizures |
| PTEN hamartoma tumour syndrome (Cowden) | Multiple facial/trunk lipomas | Thyroid/breast cancer risk |
| Gardner syndrome | Intra-abdominal lipomas | Colon polyps/cancer |
| MEN 2B | Multiple neuromas + lipomas | Medullary thyroid carcinoma |
| Dercum disease | Painful lipomas (adiposis dolorosa) | Obesity, fatigue; women > men |
Painful multiple lipomas suggest angiolipomas (vascular subtype) or Dercum disease.
Types of lipoma
Over 13 histological variants exist, classified by location, cytology, or matrix:
- Conventional: Classic subcutaneous (80%)
- Angiolipoma: Painful, young adults, vascular
- Fibrolipoma: Fibrous bands
- Myxolipoma: Mucinous stroma
- Spindle cell lipoma: Neck/shoulder, men 45-65y
- Pleomorphic lipoma: Similar sites; floret cells
- Intramuscular/intermuscular: Deep, symptomatic
- Encapsulated: Discrete capsule
- Diffuse: Infiltrative, no capsule
- Liposarcoma mimics: Atypical/infiltrating
Internal lipomas (e.g., colonic, cardiac) are rarer.
Complications
Lipomas are benign with excellent prognosis:
- Rare: Pain/numbness from compression; cosmetic disfigurement; restricted motion (large intramuscular).
- Extremely rare: Malignant transformation (<1%); local recurrence post-incomplete excision (5-10% with liposuction).
- Large lesions (>5-10 cm) require sarcoma exclusion.
How is lipoma diagnosed?
Diagnosis is clinical for typical subcutaneous lesions. Atypical features (rapid growth, pain, deep fixation, size >5 cm, multiplicity) prompt:
- Ultrasound: Homogeneous hyperechoic mass, no Doppler flow.
- MRI: Gold standard; T1/T2 hyperintense, thin capsule.
- Biopsy: Core/excisional if sarcoma suspicion.
No routine blood tests needed.
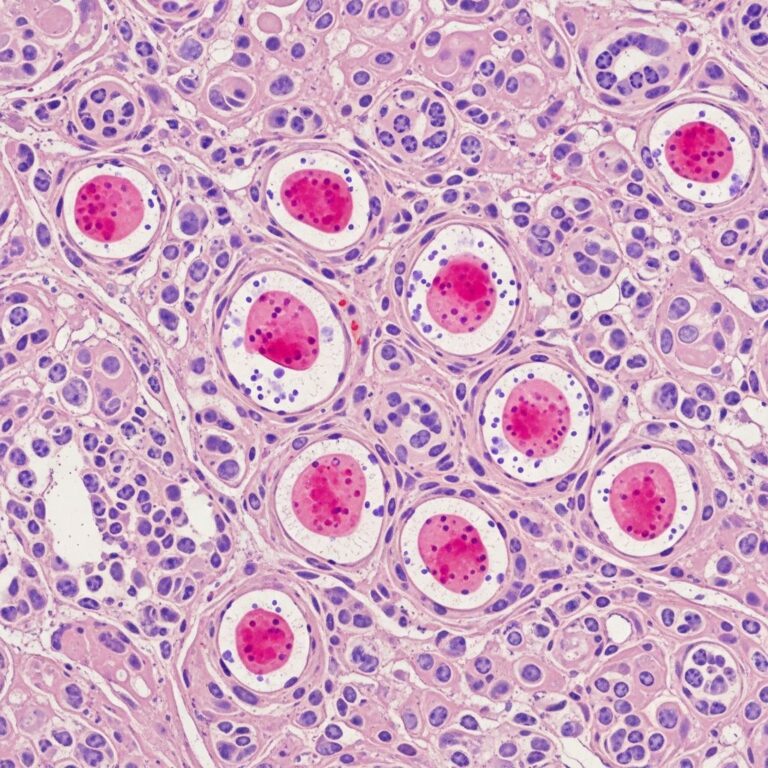
What is the pathology of lipoma?
Microscopy reveals lobulated mature adipocytes with peripheral nuclei, scant capillaries in fibrous septa, and thin capsule. Variants show:
- Angiolipoma: Capillary proliferation.
- Spindle cell: Bipolar cells.
- Fibrous: Dense collagen.
Differential includes normal fat (lacks encapsulation), liposarcoma (atypia, MDM2+), fat necrosis (ghost cells). Liberal sampling essential.
What is the treatment for lipoma?
Asymptomatic lipomas require no intervention (watchful waiting). Indications for removal:
- Symptoms (pain, compression).
- Cosmetic concerns.
- Diagnostic uncertainty.
Surgical excision: Curative; complete capsule removal minimises recurrence (<2%).
Liposuction/laser lipolysis: Good cosmesis for large/multiple; higher recurrence (up to 20%) as capsule remains.
Emerging: Injection lipolysis (deoxycholate), radiofrequency; limited evidence.
Primary care excision feasible for small, uncomplicated lesions.
Prevention
No established prevention. Weight management and trauma avoidance unproven.
Outcome
Excellent; local recurrence rare post-excision. Malignant change negligible. Syndromic cases need holistic management.
Frequently Asked Questions
Are lipomas cancerous?
No, lipomas are benign. Sarcoma risk <0.1%; biopsy large/rapidly growing lumps.
Do lipomas go away?
Rarely spontaneously; stable or slowly grow.
Should I remove my lipoma?
Only if symptomatic or cosmetic issue. Risks include scarring, recurrence.
Can lipomas be multiple?
Yes, 5-10%; screen for syndromes if >10 or familial.
Is liposuction better than excision?
Better cosmesis but higher recurrence.
References
- Dercum Disease (adiposis dolorosa) — DermNet NZ. 2023. https://dermnetnz.org/topics/dercum-disease
- Lipoma (fatty lumps) — DermNet NZ. 2024-01-15. https://dermnetnz.org/topics/lipoma
- Lipoma pathology — DermNet NZ / Assoc Prof Patrick Emanuel. 2013-05-01. https://dermnetnz.org/topics/lipoma-pathology
- Lipoma: Types, Pictures, Causes, Symptoms, Treatment — Healthline (reviewed by medical professionals). 2023-11-20. https://www.healthline.com/health/skin/lumps
- Benign Lesion (Lipoma, Cyst etc.) Guidelines — NHS Lothian. 2024. https://apps.nhslothian.scot/refhelp/guidelines/dermatology/benign-lesion-lipoma-cyst-haemangiona-xanthelasma-comedones-granuloma/
Similar Articles






Read full bio of medha deb