Malassezia (Pityrosporum) Folliculitis Pathology
Detailed pathology of Malassezia folliculitis: yeast invasion, suppurative inflammation, and diagnostic challenges in skin biopsies.
 Folliculitis Pathology")
Malassezia folliculitis, also known as pityrosporum folliculitis, represents a yeast-driven infection targeting the pilosebaceous unit, primarily attributed to lipophilic yeasts such as Malassezia globosa, M. restricta, and M. sympodialis. These yeasts are commensal on human skin but proliferate under conditions favoring overgrowth, leading to follicular inflammation.
Authoritative introduction to pathology
The pathology of Malassezia folliculitis centers on suppurative folliculitis predominantly affecting the infundibular portion of the hair follicle. Follicular occlusion often precedes or accompanies yeast proliferation, creating an environment conducive to infection. Patients typically present with monomorphic papulopustules on the upper trunk, face, and arms, mimicking acne vulgaris or bacterial folliculitis.
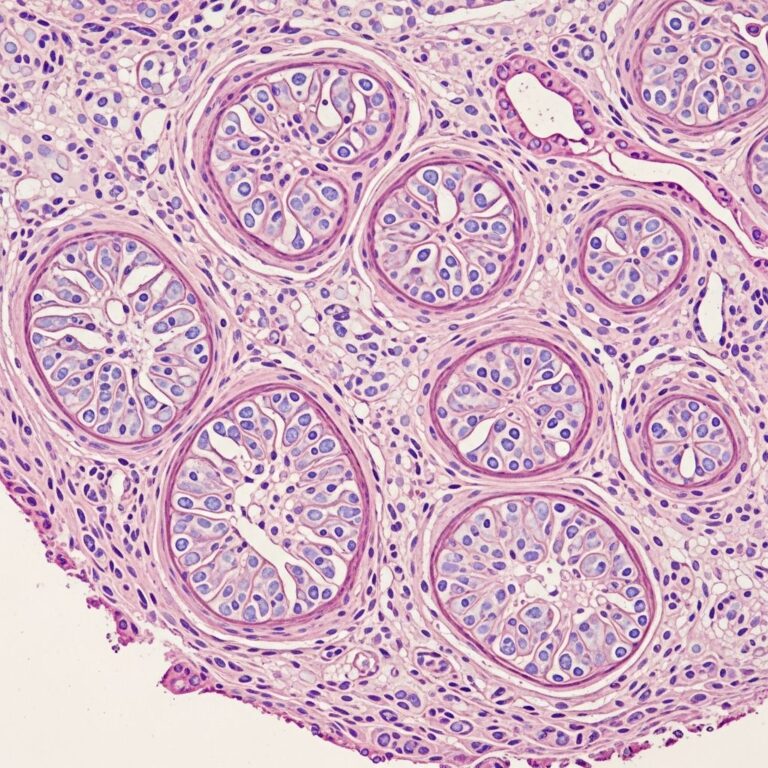
Histologically, the epidermis shows minimal changes beyond follicular plugging with keratin and debris. The key feature is intense neutrophilic infiltration within the follicle lumen, forming microabscesses. Perifollicular inflammation includes lymphocytes, histiocytes, and occasionally neutrophils, which can become exuberant if follicular rupture occurs, spilling contents into the dermis.
Causative organism and pathogenesis
Malassezia globosa is implicated in the majority of cases, thriving in lipid-rich sebum via lipases that hydrolyze triglycerides into free fatty acids for nutrition. Transition from saprophytic yeast to pathogenic hyphal forms is triggered by heat, humidity, sweating, oily skin, antibiotics, immunosuppression, or increased androgens altering sebum composition.
- Lipophilic yeasts colonize the stratum corneum and follicular infundibulum.
- Overgrowth causes dilation, keratin plugging, and wall rupture.
- Inflammatory cascade: neutrophils dominate early, followed by mixed infiltrate.
- Opportunistic nature explains associations with athletes, tropical climates, and antibiotic use.
These yeasts constitute 50-80% of the skin mycobiome normally but cause disease when ecological balance shifts.
Histopathological features
Low-power microscopy reveals dilated follicles packed with neutrophils and debris, often with a reticular keratin pattern. Higher magnification highlights oval yeast-like organisms budding within the follicle and dermis. A distinctive “clown nose” appearance describes the yeasts: thick-walled oval bodies (3-8 μm) with small unilateral buds connected by broad bases, resembling a clown’s nose and hat.
Surrounding dermis exhibits reactive changes: mild edema, dilated vessels, and mixed inflammation. Rupture leads to granulomatous response with histiocytes and multinucleated giants in chronic cases.
| Feature | Description | Significance |
|---|---|---|
| Follicular plugging | Keratin, debris, neutrophils in infundibulum | Primary occlusion promoting yeast growth |
| Suppurative inflammation | Neutrophils forming microabscesses | Hallmark of acute folliculitis |
| Yeast morphology | Oval yeasts with budding (“clown nose”) | Diagnostic on PAS/GMS stains |
| Perifollicular infiltrate | Lymphocytes, histiocytes ± rupture | Indicates chronicity or complication |
| Epidermal changes | Minimal; occasional spongiosis | Differentiates from interface dermatitides |
Special stains and microscopy
Routine H&E stains may miss yeasts due to their subtlety; PAS (periodic acid-Schiff) or GMS (Gomori methenamine silver) are essential, staining fungal walls magenta or black against the pale follicle contents. Yeasts appear numerous, clustered in the follicle lumen and dermal spill.
- PAS: Highlights glycogen-rich walls; preferred for Malassezia.
- GMS: More sensitive for sparse organisms.
- Direct microscopy (KOH prep): Spaghetti-and-meatball pattern (hyphae + yeasts).
- Culture: Lipid-supplemented media required for lipophilic species.
Dermoscopy may show perifollicular scaling or yellow dots, aiding clinical suspicion.
Differential diagnosis
Malassezia folliculitis is frequently underdiagnosed, as special stains are not routine in suppurative folliculitis biopsies. Key differentials include:
| Condition | Key Distinguishing Features | Stains/Tests |
|---|---|---|
| Bacterial folliculitis | Gram+ cocci (Staph); deeper involvement possible | Gram stain (positive); PAS/GMS negative for yeast |
| Majocchi granuloma | Dermatophyte hyphae/arthroconidia; deep granulomatous | PAS/GMS shows septate hyphae, not yeasts |
| Acne vulgaris | Comedones, rupture with squamous debris; Propionibacterium | No yeasts; clinical history key |
| Steroid acne | Monomorphic; lacks organisms | Negative stains; history of steroids |
| Eosinophilic folliculitis | Eosinophils prominent; HIV association | No fungi; perifollicular flame figures |
Bacterial folliculitis appears identical without yeasts on special stains. Majocchi shows fungal elements but hyphal, not yeast-dominant.
Clinical correlations and diagnostic pitfalls
Clinically, lesions are itchy, uniform papulopustules without comedones, resisting antibiotics but responding rapidly to antifungals (e.g., oral fluconazole, ketoconazole). This therapeutic trial supports diagnosis. Biopsy is gold standard when clinical overlap confuses: perform PAS/GMS on all suppurative folliculitis cases to avoid missing Malassezia.
Risk factors amplify suspicion: young adults, hot/humid climates, athletes, oily skin, recent antibiotics/steroids, immunosuppression.
Advanced pathological insights
Electron microscopy reveals yeast adhesion to keratinocytes via fibrillar attachments, with phospholipases inducing keratinocyte apoptosis and inflammation. Molecular studies confirm M. globosa dominance via PCR of biopsies. Chronic cases show fibrosis and scarring, rare but significant.
Quantitative histology notes higher yeast density in lesional vs. normal skin, correlating with symptom severity.
Frequently Asked Questions (FAQs)
Q: What is the hallmark histological feature of Malassezia folliculitis?
Suppurative infundibulitis with PAS-positive oval budding yeasts showing “clown nose” morphology.
Q: Why are special stains mandatory?
Yeasts are often overlooked on H&E; PAS/GMS confirm Malassezia, distinguishing from bacterial causes.
Q: How does it differ from bacterial folliculitis pathologically?
Identical inflammation but presence of yeasts vs. Gram-positive bacteria.
Q: Is follicular rupture common?
Frequent, leading to dermal spill and mixed inflammation; exuberant in severe cases.
Q: What confirms underdiagnosis?
Routine staining of folliculitis biopsies reveals Malassezia in many presumed bacterial cases.
Prognosis and management notes for pathologists
Excellent with antifungals; recurrence common due to persistent spores. Path reports should highlight yeast morphology, stain results, and recommend antifungals over antibiotics.
References
- Malassezia (pityrosporum) folliculitis — DermNet NZ. 2023. https://dermnetnz.org/topics/malassezia-folliculitis
- Pityrosporum Folliculitis — Dermatology Advisor. 2024-01-15. https://www.dermatologyadvisor.com/ddi/pityrosporum-folliculitis/
- Malassezia (Pityrosporum) Folliculitis — PMC (PubMed Central). 2014-03-01. https://pmc.ncbi.nlm.nih.gov/articles/PMC3970831/
- Malassezia (pityrosporum) folliculitis pathology — DermNet NZ. 2023. https://dermnetnz.org/topics/malassezia-pityrosporum-folliculitis-pathology
- Pityrosporum (Malassezia) Folliculitis: Causes & Treatment — Cleveland Clinic. 2024-06-10. https://my.clevelandclinic.org/health/diseases/22833-pityrosporum-folliculitis
- Folliculitis — DermNet NZ. 2023. https://dermnetnz.org/topics/folliculitis
Similar Articles






Read full bio of medha deb