Melanocytic Naevus: Complete Guide To Causes, Types, Treatment
Comprehensive guide to moles: causes, types, diagnosis, treatment, and prevention of melanocytic naevi.

A
melanocytic naevus
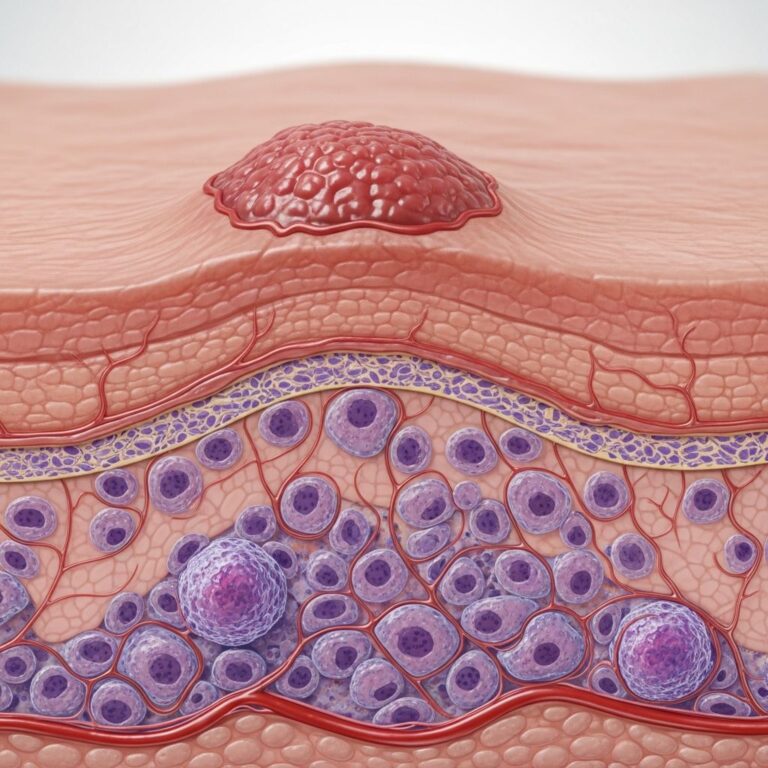
, commonly known as a mole or pigmented naevus, is a benign skin lesion resulting from the local proliferation of melanocytes, the pigment-producing cells in the skin. These lesions are extremely common, affecting most individuals, and typically appear during childhood and adolescence, often influenced by sun exposure.What is a melanocytic naevus?
Melanocytic naevi are non-cancerous growths composed of clusters of melanocytes. They can be flat (macular) or raised (papular/nodular) and vary in color from light brown to black due to melanin content. While most are harmless, changes in size, shape, or color may signal malignancy, such as melanoma. Acquired naevi develop after birth, whereas congenital ones are present at birth. Histologically, they feature nests of melanocytes at the dermoepidermal junction or within the dermis.
Who gets melanocytic naevi?
Almost everyone develops melanocytic naevi, with peak numbers occurring between ages 20 and 30. Fair-skinned individuals and those with a history of intense sun exposure tend to have more naevi. Genetic factors, including mutations like BRAF V600E, play a role in their formation. The average adult has 10–40 moles, though numbers decline after age 50 as some regress naturally. Children and adolescents are particularly prone to new naevi appearing in sun-exposed areas.
Causes
The primary cause is a genetic mutation in melanocytes, often a point mutation in the
BRAF gene
(V600E variant), triggered by ultraviolet (UV) radiation from sun exposure, especially in childhood. This leads to uncontrolled proliferation forming nests of cells. Other factors include:- Genetic predisposition and proto-oncogenes like c-met and c-kit.
- Hepatocyte growth factor influencing melanocyte migration during fetal development for congenital types.
- Age-related evolution: naevi start junctional (flat), become compound (raised), and may regress intradermally.
Sun exposure accelerates naevus formation and darkening, particularly in genetically susceptible individuals.
Clinical features
Melanocytic naevi present as well-defined, round or oval lesions ranging from 1–6 mm in diameter, though larger ones exist. Colors range from tan to black; textures from smooth macules to verrucous papules. Common sites include sun-exposed areas like the face, arms, and trunk.
- **Flat moles**: Junctional naevi, uniform pigmentation.
- **Raised moles**: Compound or intradermal, may have hair.
- Symptoms: Usually asymptomatic, but may itch or bleed if irritated.
Larger congenital naevi can be bumpy, hairy, or prone to ulceration due to deep melanocyte nests weakening skin structure.
Types of melanocytic naevi
Classification is based on clinical appearance, location of melanocyte nests, and dermoscopic patterns.
Acquired naevi (postnatal)
Develop after birth, most common type.
- Junctional naevus: Flat, pigmented macule; nests at dermoepidermal junction. Oval/cuboidal cells with clear cytoplasm.
- Compound naevus: Central papule with peripheral macule; nests in junction and dermis. Shows maturation (smaller, less pigmented cells deeper).
- Intradermal naevus: Dome-shaped, often non-pigmented (especially facial); dermal nests only. May neurotise (spindle-shaped) or show fatty/bone differentiation rarely.
Special types
- Meyerson naevus: Naevus with eczematous halo; spongiotic dermatitis histologically.
- Halo (Sutton) naevus: Central naevus with depigmented halo; lymphocytic destruction, may link to vitiligo.
- Spitz naevus: Pink/brown dome in children; epithelioid cells.
- Reed naevus: Dark spindle-cell mole on limbs.
- Balloon cell naevus: >50% large clear cells; non-distinctive clinically.
- Acral naevus (MANIAC): Pagetoid spread on soles/palms; nested, matures dermally, unlike melanoma.
- Auricular/ankle naevi: Atypical epidermal proliferation; benign with maturation.
Congenital melanocytic naevi
Present at birth or soon after; sized small (<1.5 cm), medium (1.5–20 cm), giant (>20 cm). Globular dermoscopy pattern common; deeper extension around adnexa. Prone to itch, fragility, hairiness at puberty.
Diagnosis
Diagnosis relies on clinical exam, dermoscopy, and histopathology if suspicious. Use
ABCDE rule
for melanoma risk: Asymmetry, Border irregularity, Color variation, Diameter >6 mm, Evolving.- Dermoscopy: Reveals patterns like globules (congenital), reticular, structureless. Symmetry aids benignity.
- Histology: Confirms nest location, maturation, atypia absence.
- Biopsy: Excisional for changing lesions; avoid partial in atypical sites.
Differentiate from seborrhoeic keratosis, basal cell carcinoma, melanoma.
Complications
Most benign, but risks include:
- Trauma/Irritation: Bleeding, infection from rubbing.
- Cosmetic concerns: Especially visible/large congenital naevi impacting self-image.
- Malignant transformation: Rare (<1%) for common naevi; higher (5–20%) for giant congenital to melanoma/neurocutaneous melanosis.
- Neurocutaneous melanosis: Leptomeningeal melanocytes with giant naevi; neurological risks.
| Type | Melanoma Risk | Notes |
|---|---|---|
| Common acquired | <0.1% | Very low |
| Small congenital | ~2.5% | Lifetime |
| Medium/giant congenital | 5–20% | Monitor closely |
Treatment
Observation suffices for stable naevi. Removal indicated for suspicion, symptoms, or cosmetics.
- Excision: Shave, punch, or elliptical for histopathology.
- Laser: Ablation for small/cosmetic; risks scarring/pigmentation change.
- Curettage: Intradermal naevi.
- Congenital: Staged excision or tissue expanders for large; not routine due to risks.
Avoid unnecessary removal to prevent scars.
Prevention
Minimize UV exposure:
- Sunscreen (SPF 30+), clothing, shade.
- Avoid peak sun (10am–4pm), tanning beds.
- Self-monitoring for changes; annual dermatologist checks for high-risk.
Outlook
Excellent for most; many regress post-50. Congenital may evolve but require surveillance. Early detection ensures favorable prognosis even if malignant.
Frequently Asked Questions (FAQs)
Q: Are all moles cancerous?
A: No, most melanocytic naevi are benign. Only changing ones need evaluation.
Q: When should I worry about a mole?
A: Use ABCDE: asymmetry, irregular borders, varied color, >6mm, evolving. See a dermatologist promptly.
Q: Can moles be removed safely?
A: Yes, via excision or laser by professionals; monitor for recurrence.
Q: Do congenital moles always need removal?
A: No, unless symptomatic or high-risk (giant); weigh scarring risks.
Q: How does sun exposure affect moles?
A: Increases number, size, and melanoma risk; protect skin always.
References
- Melanocytic naevi pathology — DermNet NZ. 2023. https://dermnetnz.org/topics/melanocytic-naevi-pathology
- Moles (melanocytic naevi, pigmented nevi) — DermNet NZ. 2023. https://dermnetnz.org/topics/melanocytic-naevus
- Congenital melanocytic naevi — DermNet NZ. 2023. https://dermnetnz.org/topics/congenital-melanocytic-naevi
- Intradermal and Compound Naevi (Moles) — Patient.info. 2024-01-15. https://patient.info/doctor/dermatology/intradermal-and-compound-naevi
- Melanocytic naevi: new classification — DermNet NZ. 2023. https://dermnetnz.org/cme/dermoscopy-course/melanocytic-naevi-new-classification
- Giant Congenital Melanocytic Nevus — NORD (rarediseases.org). 2023-05-01. https://rarediseases.org/rare-diseases/giant-congenital-melanocytic-nevus/
Similar Articles






Read full bio of Sneha Tete