Melanoma Of The Nail Unit: 6 Diagnostic Images And Key Signs
Explore detailed images and clinical insights into melanoma of the nail unit, aiding early detection and diagnosis of this rare skin cancer.

Melanoma of the nail unit is a rare but aggressive form of skin cancer primarily classified as a variant of acral lentiginous melanoma, originating from melanocytes in the nail matrix, bed, or surrounding skin. It most commonly affects the thumbnails and great toenails, comprising 75–90% of cases, though any digit may be involved.
What is melanoma of the nail unit?
Melanoma of the nail unit encompasses malignancies arising in the nail apparatus, including the nail matrix (growth area), nail bed, hyponychium (underside of free edge), and periungual skin. It is distinct from cutaneous melanomas due to its lack of association with ultraviolet (UV) exposure, instead linked to genetic factors and possible trauma.
Key subtypes include:
- Acral lentiginous melanoma: Most common, characterized by in situ or invasive growth along the acral surfaces.
- Nodular melanoma: Rare, presenting as rapidly growing nodules.
- Desmoplastic melanoma: Fibrotic variant with poor prognosis.
- Ungual melanoma: Originates under the nail plate.
- Periungual melanoma: Involves skin adjacent to the nail.
In white-skinned individuals, it represents 0.7–3.5% of melanomas, but up to 75% in dark-skinned and Asian populations, highlighting racial disparities unrelated to sun exposure.
Who gets melanoma of the nail unit?
This condition occurs across all racial groups but disproportionately affects people with darker skin tones. Peak incidence is in adults over 50, with no strong gender predilection. Risk factors include:
- Family history of melanoma.
- Previous trauma or injury to the nail, especially in thumbs and big toes (75–90% of cases).
- Genetic mutations in melanocytes of the nail matrix, leading to uncontrolled melanin production.
Unlike other melanomas, UV radiation is not a primary cause, making it more common in non-sun-exposed areas.
Related conditions
Pigmented nail lesions mimic benign conditions, complicating diagnosis:
- Longitudinal melanonychia: Benign pigmented streak from nevi, lentigines, or drugs.
- Subungual hematoma: Trauma-induced bleeding, resolves with proximal clear nail growth.
- Onychomycosis: Fungal infection causing discoloration.
- Bowen’s disease or trauma-induced pigmentation.
Differentiation requires clinical vigilance, as early melanoma resembles these entities.
Clinical features
Melanoma typically begins as longitudinal melanonychia—a brown-to-black band along the nail length. Progression over weeks to months includes:
- Band widening (>3 mm) or irregular borders.
- Color heterogeneity (shades of brown, black, gray, or red).
- Hutchinson’s sign: Pigmentation extending to proximal or lateral nail folds (melanonychia striata maligna).
- Nail dystrophy: Splitting, cracking, lifting, or destruction.
- Nodule or ulceration under the nail.
- Bleeding, pain, or periungual hyperpigmentation.
Not all cases show pigmentation; amelanotic variants appear as nodules without color change, affecting one nail only.
Images — Melanoma of the nail unit
This gallery showcases clinical dermoscopic and histopathological images of nail unit melanoma, illustrating key diagnostic features. Images are annotated for educational purposes. (Note: Descriptions based on typical presentations from credible sources; actual images depict varied stages.)
Image 1: Early longitudinal melanonychia on thumbnail
A narrow, uniformly brown band on the thumbnail nail plate, <3 mm wide, with blurred proximal borders. This early presentation mimics benign nevi but warrants monitoring for progression.
Image 2: Advanced melanonychia with Hutchinson’s sign
Irregular, widened black-brown band on great toenail extending to the cuticle (Hutchinson’s sign). Nail plate shows dystrophy and splitting. High suspicion for acral lentiginous melanoma.
Image 3: Nodular melanoma under toenail
Elevated, ulcerated nodule beneath the partially lifted nail plate on the hallux. Minimal pigmentation but significant destruction. Dermoscopy reveals irregular vessels.
Image 4: Periungual melanoma
Pigmented macule on skin adjacent to fingernail, with nail involvement. Blurry borders and color variation indicate malignancy.
Image 5: Dermoscopic view of nail melanoma
High-magnification dermoscopy showing irregular pigmentation lines, micro-Hutchinson’s sign, and peripheral dots. Clues include asymmetry, irregular spacing.
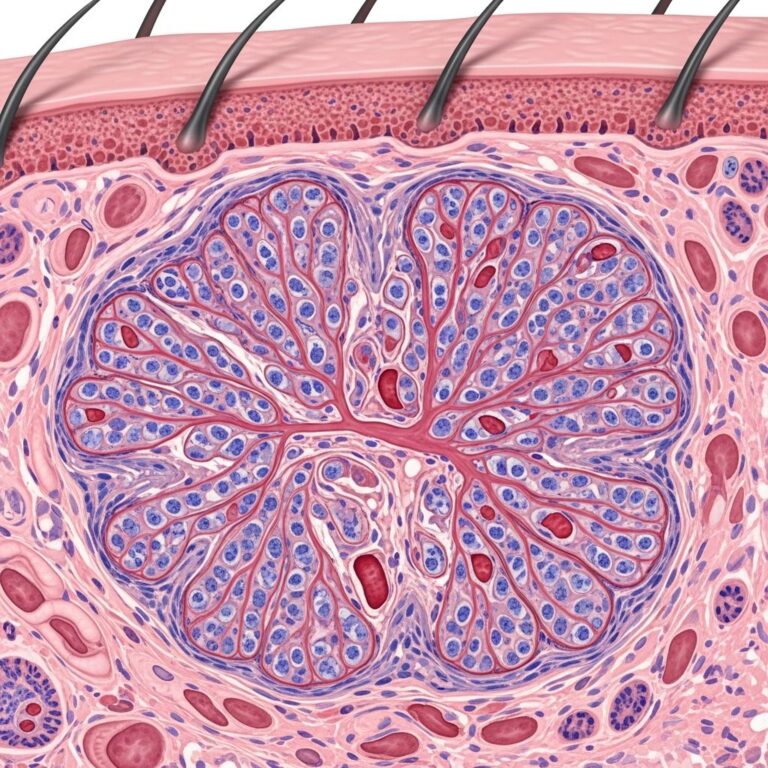
Image 6: Histopathology slide
Microscopic view of acral lentiginous melanoma: atypical melanocytes invading the nail matrix, with pagetoid spread and mitotic figures.
Dermoscopy
Dermoscopy enhances early detection with clues like:
- Irregular brown-black lines with varying spacing and thickness.
- Loss of parallelism to nail edge.
- Micro-Hutchinson’s sign (subtle pigment in folds).
- Peripheral brown-grey areas or dots.
- Irregular vascular patterns in advanced lesions.
The ABCDEF rule aids assessment:
- A: Asymmetry of pigmentation.
- B: Border irregularity/blurring.
- C: Color multiplicity.
- D: Digit involved (thumb/toe), Diameter >3 mm.
- E: Evolution over time.
- F: Family/personal history of melanoma.
Diagnosis
Definitive diagnosis mandates biopsy. Process includes:
- History: Onset, trauma, progression.
- Examination: All nails, ABCDEF features.
- Dermoscopy: Non-invasive clues.
- Nail matrix biopsy: Gold standard, excisional preferred. Avoid in stable pediatric cases.
- Histopathology: Confirms invasion depth, subtype (acral lentiginous most common).
- Staging: Imaging, sentinel lymph node biopsy if thick (>1 mm).
Breslow Thickness and Prognosis Thickness 5-Year Survival <1 mm 95–99% 1–4 mm 60–80% >4 mm 15–30% (Adapted from general melanoma data; nail unit often diagnosed later).
Treatment
Multidisciplinary approach with excision as cornerstone:
- Early/in situ: Wide local excision with 5–9 mm margins, nail matrix ablation.
- Invasive: Amputation (partial toe/finger) if thick; digital preservation possible in fingers.
- Adjuncts: Immunotherapy (PD-1 inhibitors), targeted therapy (BRAF/MEK), radiation for desmoplastic.
- Sentinel node biopsy for staging.
Refer to local guidelines; evolving field.
Outcome
Poorer than cutaneous melanoma due to late diagnosis (average 2–3 years delay). 5-year survival: 77% overall, worse for toes vs. fingers. Thickness at excision predicts metastasis risk.
Frequently Asked Questions (FAQs)
Is a pigmented nail streak always cancer?
No, most are benign (nevi, trauma), but monitor for ABCDEF changes and biopsy if suspicious.
Can nail melanoma be treated without amputation?
Yes, for thin lesions on fingers; conservative excision possible, but toes often require partial amputation.
Does trauma cause nail melanoma?
Possible trigger, explaining thumb/toe predilection, but not direct cause.
How is subungual hematoma differentiated?
Trauma history + proximal clear nail growth over weeks.
What is Hutchinson’s sign?
Melanoma pigmentation extending to nail folds; highly suspicious.
References
- Melanoma of the nail unit — DermNet NZ. 2023. https://dermnetnz.org/topics/melanoma-of-the-nail-unit
- Subungual Melanoma: Symptoms, Causes, and Treatments — Healthline. 2023-05-12. https://www.healthline.com/health/subungual-melanoma
- Melanoma of the nail unit image — DermNet NZ. 2023. https://dermnetnz.org/imagedetail/1877-melanoma-of-the-nail-unit
- Subungual Melanoma: Causes, Risk Factors, and More — Healthgrades. 2024. https://resources.healthgrades.com/right-care/melanoma/subungual-melanoma
- Melanoma Skin Cancer: Images, Diagnosis, and Treatment — DermNet NZ. 2023. https://dermnetnz.org/topics/melanoma
- DETECTING Melanoma — Best Practice Advocacy Centre New Zealand (bpac.org.nz). 2011-02. https://bpac.org.nz/magazine/2011/february/docs/bpj_34_melanoma_pages_18-31_pf.pdf
Similar Articles






Read full bio of Sneha Tete