Meningioma Grading: Understanding Types, Treatment, and Prognosis
Comprehensive guide on meningioma grading: diagnosis, treatment options, and outcomes to improve patient care.

Introduction to Meningioma Grading
Meningiomas are tumors that arise from the meninges, which are the protective membranes surrounding the brain and spinal cord. Although the majority of meningiomas are benign and slow-growing, they can vary in aggressiveness and behavior. To assess their potential impact and guide treatment decisions, meningiomas are assigned a grade that reflects their severity, cellular features, and growth rates.
This article outlines the meningioma grading system, the characteristics of different tumor grades, diagnostic approaches, treatment options, and prognosis.
What Are Meningiomas?
Meningiomas develop from the meninges layer surrounding the brain and spinal cord. They represent the most frequent primary tumor of the central nervous system. Although often benign, these tumors can sometimes display atypical or malignant characteristics, complicating treatment and increasing recurrence risks.
These tumors primarily grow on the surface of the brain but can, depending on size and location, exert pressure on the brain tissue, potentially causing neurological symptoms.
Meningioma Causes and Risk Factors
- Genetic Mutations: Most meningiomas arise due to genetic mutations, which usually occur spontaneously but can also be inherited, as in genetic disorders like neurofibromatosis type 2, Von Hippel-Lindau disease, or Cowden syndrome.
- Age: Risk increases with age, particularly in individuals over 65 years.
- Gender and Hormones: Women develop meningiomas more frequently than men, potentially linked to hormonal factors. Hormone replacement therapy and certain birth control methods, such as Depo-Provera, have been associated with a higher risk of developing meningiomas.
The Meningioma Grading System
Meningiomas are classified into three grades (I to III) based on how tumor cells look under the microscope, reflecting their growth behavior and aggressiveness.
| Grade | Description | Characteristics | Prognosis |
|---|---|---|---|
| Grade I | Benign meningiomas | Slow-growing, distinct borders, noncancerous, rare spread to other body parts | Good prognosis, often curable by surgery alone |
| Grade II | Atypical meningiomas | Displays abnormal cellular characteristics, grows faster than grade I, higher recurrence rates after treatment | Intermediate prognosis; potential malignancy if untreated |
| Grade III | Malignant (anaplastic) meningiomas | Highly aggressive, invades surrounding brain tissue, rapid growth, difficult to remove completely | Poor prognosis, high recurrence and mortality rates |
Diagnosis and Classification of Meningiomas
The diagnosis and grading of meningiomas depend on imaging and histopathological evaluation:
- Imaging: Magnetic resonance imaging (MRI) is the gold standard for initial detection and evaluation. Advanced imaging techniques like Amide Proton Transfer (APT) MRI are emerging tools used to help differentiate meningioma grades based on tumor characteristics.
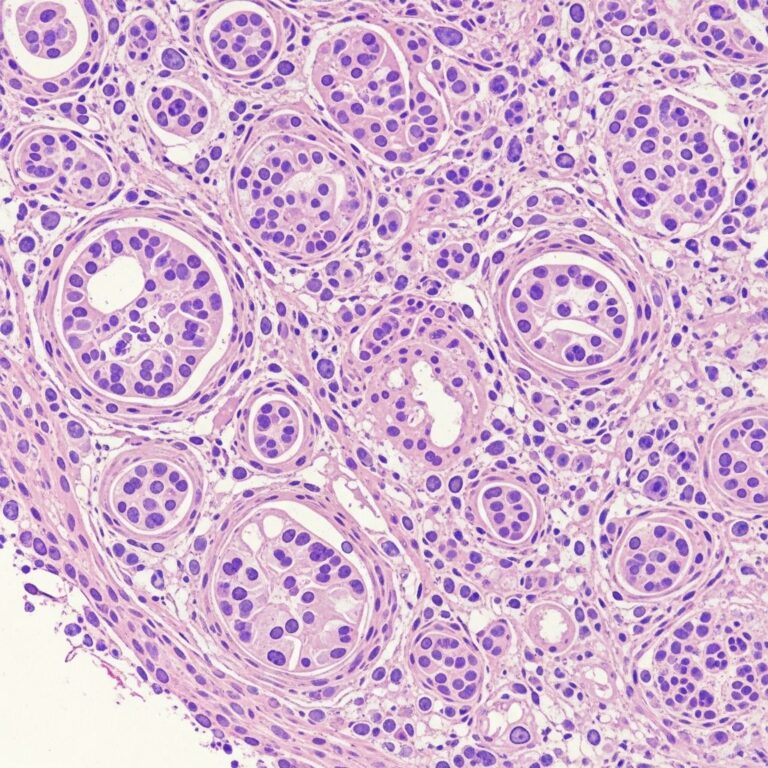
- Histopathology: A tissue biopsy or surgical resection specimen is microscopically examined to study cellular details that determine the WHO grade.
- Molecular and Protein Markers: Recent research identifies specific proteins such as NY-ESO-1 expressed predominantly in high-grade meningiomas, offering potential targets for novel therapies and better prognostic tools.
Treatment Options by Grade
Treatment strategies vary depending on the tumor grade, size, location, and patient factors.
Grade I Meningiomas
- Surgical Removal: Most Grade I tumors can be effectively treated with complete surgical excision.
- Observation: Small, asymptomatic tumors may be monitored periodically using MRI.
- Radiotherapy: Usually not required unless the tumor recurs or cannot be fully removed.
Grade II Meningiomas
- Surgery: Attempted to remove as much tumor as possible.
- Radiation Therapy (RT): Often recommended postoperatively due to higher recurrence rates. Conventional fractionated RT delivering a total dose of approximately 59.4 Gy is common post-resection.
- Stereotactic Radiosurgery (SRS): Considered for small residual tumors or patients unable to undergo standard radiation courses, though less preferred compared to conventional RT.
Grade III Meningiomas
- Aggressive Surgical Resection: Challenging due to invasive growth but remains a primary approach.
- Adjuvant Radiation: Essential due to aggressive nature and tendency to recur.
- Experimental Therapies: Research into immunotherapies targeting specific proteins like NY-ESO-1 holds promise but remains investigational.
Emerging Research and Therapeutic Targets
Scientists at Johns Hopkins and other institutions have discovered that nearly 100% of high-grade meningiomas express the NY-ESO-1 protein, a cancer antigen offering avenues for immunotherapy. This finding has accelerated efforts to repurpose or develop treatments targeting this protein, potentially improving outcomes for aggressive meningioma types resistant to conventional therapies.
Prognosis and Recurrence Risks
Meningioma prognosis depends largely on tumor grade, completeness of resection, and adjuvant therapy:
- Grade I: Usually excellent prognosis with surgical treatment and low recurrence rates (~9%).
- Grade II: Intermediate prognosis with recurrence reported up to 28%. Continuous follow-up and adjuvant treatment are critical.
- Grade III: Poor prognosis; recurrence rates can reach 75% or higher, demanding aggressive multimodal treatment and close surveillance.
Frequently Asked Questions (FAQs)
Q: How are meningiomas graded?
A: Meningiomas are graded by the World Health Organization on a scale of I to III based on cellular features and growth behavior observed under a microscope. Grade I is benign, Grade II atypical, and Grade III malignant and aggressive.
Q: What are the common treatment options for meningiomas?
A: Treatment typically includes surgical removal, with radiation therapy recommended for higher grade tumors or incomplete resections. Emerging immunotherapies are under investigation for malignant meningiomas.
Q: Can meningiomas be cured?
A: Most Grade I meningiomas can be cured through surgery. Grade II and III tumors have higher risks of recurrence and require additional treatments and long-term monitoring.
Q: What are the symptoms of meningiomas?
A: Symptoms depend on tumor size and location; they may include headaches, seizures, vision changes, weakness, or neurological deficits.
Summary
Meningioma grading is essential to determine the tumor’s potential aggressiveness and to guide clinical management. From benign Grade I meningiomas with excellent outcomes following surgery to aggressive Grade III tumors requiring multimodal therapies, understanding the grade informs prognosis and treatment intensity.
Continuous advances in imaging, histopathology, molecular biology, and radiation oncology are improving diagnostic accuracy and expanding treatment options, including promising immunotherapies targeted at specific tumor antigens.
References
- Meningioma Grading — Shapiro Legal Group. 2025-11-20. https://www.shapirolegalgroup.com/meningioma-grading.html
- A Case-based Guide for WHO Grade 2 Meningiomas — Practical Radiation Oncology, Johns Hopkins University. 2024-11-01. https://pure.johnshopkins.edu/en/publications/a-case-based-guide-for-world-health-organization-who-grade-2-meni
- Promising Therapeutic Target for High-Grade Brain Tumors — Johns Hopkins Medicine. 2013-08-27. https://www.ludwigcancerresearch.org/news-releases/ludwig-scientists-at-johns-hopkins-find-promising-therapeutic-target-for-hard-to-treat-brain-tumor/
- APT MRI in Grading Meningiomas: A Study Overview — ES Medical Publishing. 2025-06-15. https://esmed.org/apt-mri-in-grading-meningiomas-a-study-overview/
- Types of Brain Tumors — Johns Hopkins Pathology. 2025-01-10. https://pathology.jhu.edu/brain-tumor/types
Similar Articles






Read full bio of medha deb