Mid-Dermal Elastolysis: 5 Causes, Symptoms & Treatments
Rare acquired skin disorder causing fine wrinkling due to mid-dermal elastic fibre loss, primarily affecting young women on trunk and arms.

Mid-dermal elastolysis is a rare, acquired skin condition characterised by the selective loss of elastic fibres in the mid-dermis, leading to diffuse fine wrinkling, most commonly on the trunk and upper arms.
What is mid-dermal elastolysis?
**Mid-dermal elastolysis (MDE)** is an uncommon dermatological disorder defined by the idiopathic degradation of elastic fibres specifically within the mid-reticular dermis. Elastic fibres, composed of an elastin core surrounded by fibrillin microfibrils, provide skin with its essential recoil and resilience properties. In MDE, this selective loss results in clinically apparent fine wrinkling without significant epidermal or deeper dermal changes. First described by Shelley and Wood in 1977 as ‘wrinkles due to idiopathic loss of mid-dermal elastic tissue,’ MDE predominantly affects young to middle-aged Caucasian females, with over 90% of reported cases occurring in women.
The condition is asymptomatic in most cases, though it causes significant cosmetic concern. Unlike photoageing or other elastolytic disorders, MDE spares the papillary dermis and deep dermis, creating a band-like zone of elastolysis visible on histopathology. Prevalence is low, with fewer than 200 cases documented in medical literature, underscoring its rarity.
Who gets mid-dermal elastolysis?
MDE primarily affects women aged 20–50 years, with a striking female predominance (female-to-male ratio approximately 9:1). It is most common in fair-skinned individuals of Caucasian descent, though isolated cases in other ethnicities have been reported. Common sites include the trunk (abdomen, flanks, back), upper arms, and occasionally the neck; the face, lower legs, palms, and soles are rarely involved.
Risk factors remain unclear, but associations include sun exposure, hormonal influences (e.g., oestrogen modulating matrix metalloproteinases), and autoimmune conditions like thyroid disease. No hereditary pattern is established, distinguishing MDE from congenital elastopathies.
What causes mid-dermal elastolysis?
The exact aetiopathogenesis of MDE is unknown, but several mechanisms contribute to elastic fibre destruction:
- Enzymatic degradation: Increased activity of elastases, particularly matrix metalloproteinases (MMPs) such as MMP-2 and MMP-9, leads to elastin breakdown. Fibroblasts from lesional skin show elevated elastase synthesis, with reduced tissue inhibitors of metalloproteinases (TIMPs).
- Elastophagocytosis: Macrophages phagocytose fragmented elastic fibres, as seen on electron microscopy with aberrant dense substances and loose fibril aggregates.
- Inflammatory triggers: Subtle histiocytic and lymphocytic infiltrates suggest a low-grade inflammatory process, potentially mimicking early annular elastolytic granuloma.
- Actinic damage: UV exposure may upregulate MMPs, though MDE occurs in sun-protected areas.
- Hormonal factors: Oestrogen’s role in MMP regulation implicates hormonal influences in this female-centric disease.
Lysyl oxidase (LOX) family dysfunction may impair elastin cross-linking, exacerbating fragility. Once lost, elastin turnover is minimal (half-life exceeding human lifespan), rendering damage permanent.
What are the clinical features of mid-dermal elastolysis?
MDE manifests with asymptomatic, well-demarcated patches of fine, ripple-like wrinkling resembling crêpe paper or cigarette paper. Three clinical subtypes are recognised:
- Type I (most common): Diffuse, reticulate fine wrinkles on trunk and arms, without preceding inflammation.
- Type II: Soft plaques with perifollicular papular protrusions, giving a peau d’orange appearance.
- Type III: Reticular erythema, sometimes with preceding urticarial plaques or inflammatory phase.
Lesions are non-pitting, non-scarring, and symmetrically distributed. Progression is slow, stabilising over months to years without spontaneous resolution. Rare variants include facial or thigh involvement.
Diagnosis
Diagnosis relies on clinicopathological correlation. Key features include:
- Clinical suspicion: Fine wrinkling in typical distribution in young women.
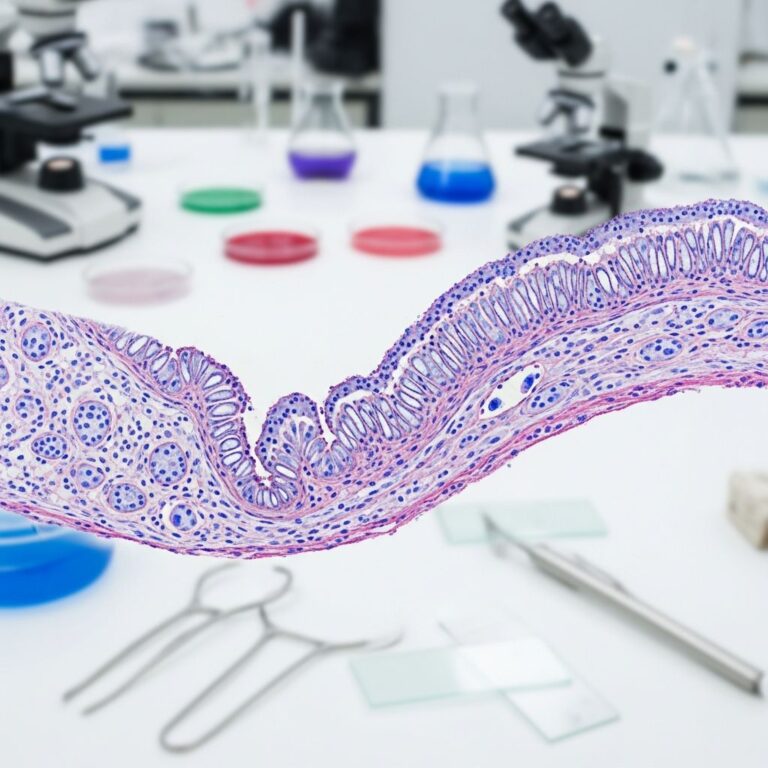
- Histopathology: Band-like absence of elastic fibres in mid-reticular dermis on elastic van Gieson (EVG) or orcein stains. Haematoxylin-eosin (H&E) may show normal epidermis, subtle perivascular lymphohistiocytic infiltrates, or elastophagocytosis. Epidermis and deep dermis are spared.
Differential diagnosis: Distinguished from anetoderma (superficial elastolysis), papillary dermal elastolysis (upper dermis), photoageing (papillary + deep changes), and pseudoxanthoma elasticum-like elastolysis (papillary involvement).
| Condition | Key Differentiator |
|---|---|
| Anetoderma | Superficial dermal elastolysis, herniation |
| Pseudoxanthoma elasticum-like papillary dermal elastolysis | Papillary dermis affected, papular |
| Photoageing | Solar elastosis, coarse wrinkles |
| Mid-dermal elastolysis | Mid-dermal band-like loss |
Treatment of mid-dermal elastolysis
No curative treatment exists; management is symptomatic and cosmetic. Options include:
- Topical retinoids (tretinoin): Promote collagen synthesis and mild elastic fibre regeneration; applied nightly.
- Systemic retinoids (acitretin): Used in extensive cases, with variable success.
- Sunscreens: Prevent exacerbation from UV-induced MMPs.
- Topical corticosteroids: For inflammatory variants (type III).
- Laser therapy (fractional CO2, Nd:YAG): Stimulates neocollagenesis; limited evidence.
- Ca channel blockers (nifedipine): Anecdotal reports of halting progression.
Treatment response is modest; most stabilise spontaneously. Patient education on cosmetic camouflage is key.
Frequently asked questions (FAQs) on mid-dermal elastolysis
What is mid-dermal elastolysis?
A rare acquired disorder causing fine skin wrinkling due to selective loss of mid-dermal elastic fibres, mainly affecting young women’s trunk and arms.
Is mid-dermal elastolysis dangerous?
No, it is benign, asymptomatic, and not associated with systemic disease, though cosmetically distressing.
How is mid-dermal elastolysis diagnosed?
By skin biopsy showing band-like mid-dermal elastolysis on EVG stain, after clinical suspicion.
Can mid-dermal elastolysis be cured?
No cure; treatments like retinoids may improve appearance but do not fully restore elastic fibres.
Does sun exposure cause it?
UV may contribute via MMP upregulation, but lesions often occur in sun-protected areas.
Is it hereditary?
No, it is acquired with no known genetic basis.
This comprehensive overview draws from peer-reviewed sources to provide authoritative insights into MDE. Early diagnosis via biopsy ensures appropriate management. Consult a dermatologist for personalised advice.
References
- Generalized mid-dermal elastolysis — PMC – NIH. 2014-10-01. https://pmc.ncbi.nlm.nih.gov/articles/PMC4211503/
- DP13: Mid‐dermal elastolysis: a study of eight cases — British Journal of Dermatology, Oxford Academic. 2022-07-01. https://academic.oup.com/bjd/article-abstract/187/S1/150/6700542
- Mid-dermal elastolysis: A female-centric disease; case report and review of the literature — PMC – NIH. 2017-05-01. https://pmc.ncbi.nlm.nih.gov/articles/PMC5418881/
- Mid-dermal elastolysis — DermNet NZ. 2014-11-01. https://dermnetnz.org/topics/mid-dermal-elastolysis
- Mid-dermal elastolysis — VisualDx. Accessed 2026. https://www.visualdx.com/visualdx/diagnosis/mid-dermal+elastolysis?diagnosisId=51485&moduleId=101
- Mid-Dermal Elastolysis on Face, Unusual Localization: A Case Report — Journal of Medical Cases. 2016-01-01. https://www.journalmc.org/index.php/JMC/article/view/1771/1140
- Mid dermal elastolysis — Dermatopathology, Weill Cornell. Accessed 2026. https://dermpath.weill.cornell.edu/diagnosis-gallery/mid-dermal-elastolysis
Similar Articles






Read full bio of Sneha Tete