Multiple Self-Healing Squamous Epitheliomas of Ferguson-Smith
Rare inherited skin disorder causing multiple self-resolving squamous-like tumors that leave characteristic pitted scars.

Authoritative fact-checked reference for multiple self-healing squamous epitheliomas of Ferguson-Smith (MSSE)
Reviewed and updated by dermatologists
What is multiple self-healing squamous epitheliomas of Ferguson-Smith?
Multiple self-healing squamous epitheliomas (MSSE), also known as Ferguson-Smith disease, is a rare inherited skin disorder characterised by the sudden onset of multiple lesions that clinically and histologically resemble well-differentiated squamous cell carcinomas (SCC) or keratoacanthomas (KA). Unlike true malignancies, these tumours are locally invasive but spontaneously regress after several months to weeks, often leaving behind distinctive pitted or crateriform scars.
This condition represents a unique paradox in dermatology: tumours that mimic aggressive skin cancers yet possess an intrinsic capacity for self-resolution. First documented in 1934, MSSE challenges conventional understandings of tumour biology, highlighting the role of genetic modifiers in tumour suppression and regression.
MSSE is classified as a rare familial skin cancer syndrome (OMIM #132800), with an estimated prevalence far below 1 in 100,000 individuals, predominantly reported in families of Scottish descent but observed worldwide.
Who gets multiple self-healing squamous epitheliomas of Ferguson-Smith (MSSE)?
MSSE follows an autosomal dominant inheritance pattern with incomplete penetrance, meaning an affected individual has a 50% chance of passing the mutation to each child, though not all carriers develop clinical symptoms.
- Age of onset: Typically adolescence to early adulthood (teens to 30s), earlier than sporadic SCC or KA.
- Sex: Affects males and females equally.
- Ethnicity/geography: Initially described in Scotland; founder effect suspected in West of Scotland families, but cases reported globally.
- Risk factors: Family history is paramount. UV exposure may trigger lesions but is not strictly required, distinguishing MSSE from typical SCC.
Penetrance approaches 90% by age 60 among TGFBR1 mutation carriers in affected pedigrees. Notably, palmar and plantar skin are spared, suggesting follicular origin.
Causes
MSSE exemplifies digenic inheritance, requiring germline loss-of-function mutations in the TGFBR1 gene (chromosome 9q22) plus permissive haplotypes at a second linked locus on 9q, likely explaining variable expressivity.
- TGFBR1 mutations: Eleven distinct heterozygous mutations identified. Wild-type TGFBR1 functions as a tumour suppressor; somatic “second hit” loss unmasks carcinogenesis, but self-healing suggests compensatory mechanisms.
- Modifier locus: Haplotype studies in founder families confirm requirement for chromosome 9q permissive variants.
- Molecular paradox: Mutant TGFBR1 impairs signalling, paradoxically promoting early tumour growth while enabling immune-mediated regression.
Transforming growth factor-β (TGF-β) pathway dysregulation is central: biphasic effects observed in skin SCC models promote initiation but enable later resolution. No environmental triggers like HPV identified.
Clinical features
Lesions emerge singly or in crops, favouring sun-exposed, trauma-prone sites: nose (most common), ears, perioral face, dorsal hands, forearms. Trunk rarely affected; palms/soles spared.
Lesion evolution (classic 4-6 month cycle):
- Weeks 1-4: Dull red macule → rapidly growing papule/nodule (1-3 cm).
- Weeks 4-8: Central umbilication, keratinous plug formation.
- Months 2-4: Plug extrusion → crateriform ulcer.
- Months 4-6: Spontaneous involution → pitted/atrophic scar.
Lifetime lesion burden varies: 1-2 (mild) to >100 (severe). Facial lesions smaller but more numerous; limb lesions larger, more destructive. Scars cause cosmetic disfigurement, particularly periorificial.
Systemic associations rare but include aortic root dilatation in some TGFBR1 mutation carriers. No metastases reported despite local invasion.
Diagnosis
Suspect MSSE in young patients with multiple SCC/KA-like lesions + family history. Diagnosis combines:
- Clinical triad: Multiple lesions, early onset (<40), self-healing.
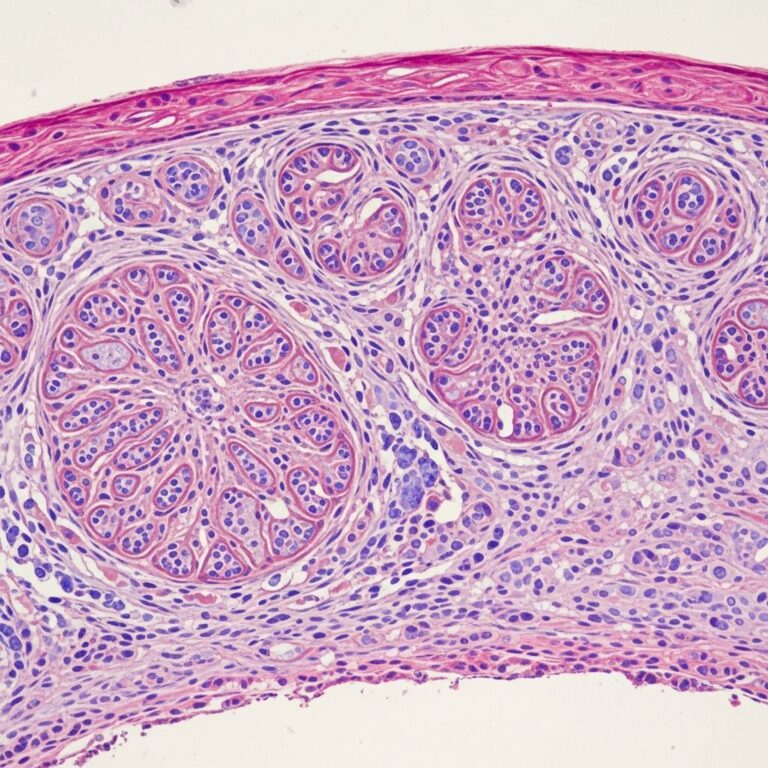
- Histology: Well-differentiated SCC pattern – invasive epithelial nests, central keratinisation, dermal fibrosis. Distinguished from KA by absent shoulder/lip abscesses.
- Genetics: Confirmatory TGFBR1 sequencing (germline heterozygous mutation).
Investigations:
- Lesional biopsy (diagnostic + excludes true SCC).
- Family pedigree analysis.
- TGFBR1 genetic testing (pathognomonic).
Differential diagnoses
| Differential | Key Distinguishing Features |
|---|---|
| Sporadic keratoacanthoma (KA) | Single lesion, older patients, perfect shouldering/lip abscesses on histology |
| Multiple self-healing epitheliomas (self-resolving SCC) | MSSE = familial/genetic; sporadic = ?HPV-related |
| Grzybowski syndrome | Generalised eruptive KA, no scarring, no genetics |
| Ferguson-Smith vs. keratoacanthoma-centric syndromes | MSSE genetic (TGFBR1); others often immune |
| True SCC | No spontaneous regression, metastases possible, solar elastosis |
Treatment
Lesions self-resolve, but intervention improves cosmesis, accelerates healing, prevents complications:
- Surgical: Excision, curettage + cautery (first-line).
- Medical: Oral retinoids (acitretin) reduce frequency.
- Intralesional: Steroids, 5-FU.
- Other: Cryotherapy, laser ablation, topical therapies.
AVOID radiotherapy: Triggers new lesions in treatment field.
Prevention: Strict sun protection (UPF50+, hats). Genetic counselling for families.
Outlook
Benign prognosis: no metastases despite invasion. Severe cases cosmetically disfiguring from cumulative scarring. Regular dermatology surveillance recommended. Oral retinoids offer prophylaxis in high-burden patients.
Understanding MSSE pathogenesis may illuminate mechanisms of spontaneous tumour regression applicable to common SCC.
Frequently asked questions about MSSE
Is MSSE a true cancer?
No. Despite SCC-like histology and local invasion, lesions universally self-resolve without metastasis.
How do I know if I have the MSSE gene?
TGFBR1 genetic testing confirms diagnosis in suspicious cases.
Will all my children get MSSE?
50% inheritance risk, but incomplete penetrance means some carriers asymptomatic.
Can sun exposure be avoided entirely?
Not required for lesion development (familial cases without UV history), but minimises triggers.
What is the scarring like?
Characteristic pitted, crateriform atrophic scars, especially periorificial.
References
- Multiple Self-Healing Squamous Epithelioma (MSSE): A Digenic … — PMC/NCBI. 2020-12-01. https://pmc.ncbi.nlm.nih.gov/articles/PMC7760568/
- Multiple self-healing squamous epitheliomas of Ferguson-Smith (MSSE) — DermNet NZ. 2023-01-01. https://dermnetnz.org/topics/multiple-self-healing-squamous-epitheliomas-of-ferguson-smith-msse
- Multiple Self-Healing Squamous Epithelioma (MSSE) — PubMed. 2020-11-30. https://pubmed.ncbi.nlm.nih.gov/33256177/
- Multiple self-healing squamous epithelioma — Orphanet. 2024-01-01. https://www.orpha.net/en/disease/detail/65748
- Multiple self-healing squamous epithelioma — NORD Rare Diseases. 2023-01-01. https://rarediseases.org/mondo-disease/multiple-self-healing-squamous-epithelioma/
- Multiple self-healing squamous epithelioma — National Cancer Institute. 2024-01-01. https://www.cancer.gov/publications/dictionaries/cancer-terms/def/multiple-self-healing-squamous-epithelioma
Similar Articles






Read full bio of medha deb