Nasal Polyps: 6 Symptoms, Causes, And Treatment Options
Understand nasal polyps: causes, symptoms, diagnosis, treatments, and prevention strategies for better sinus health.

Nasal polyps are soft, noncancerous growths that develop in the lining of the nasal passages or sinuses due to chronic inflammation. These benign swellings can vary in size from tiny and unnoticeable to large clusters that block airflow, leading to symptoms like nasal congestion, reduced sense of smell, and recurrent infections. Often associated with chronic rhinosinusitis (CRS), asthma, allergies, or conditions like cystic fibrosis, nasal polyps affect quality of life significantly if untreated. Early diagnosis and management, ranging from medications to surgery, can effectively control symptoms and prevent recurrence.
What Are Nasal Polyps?
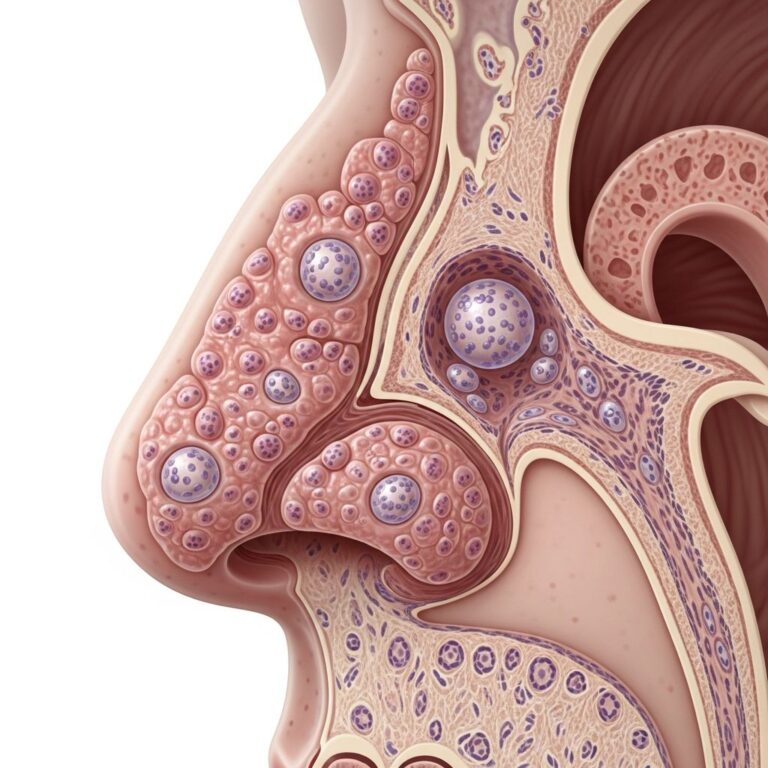
Nasal polyps are inflammatory outgrowths of the sinonasal mucosa, typically benign and hyperplastic. They most commonly occur in patients with chronic rhinosinusitis with nasal polyposis (CRSwNP), but can also appear in systemic diseases like cystic fibrosis or aspirin-exacerbated respiratory disease (AERD). These growths resemble teardrops or grapes, appearing pink or yellowish, and develop bilaterally in the nasal passages or sinuses. Small polyps may be asymptomatic, but larger ones obstruct nasal airflow, impair smell (anosmia), taste (ageusia), and cause chronic congestion. The condition stems from persistent mucosal inflammation, immune dysregulation, and epithelial barrier dysfunction, leading to edema and tissue proliferation.
Classifications include localized (reactive to inflammation or neoplasm), diffuse (linked to CRSwNP with Th2 eosinophilic inflammation), and systemic (e.g., cystic fibrosis with neutrophil-driven polyps). In Western populations, Th2-driven eosinophilia with elevated IL-5 predominates, often triggered by allergies, while cystic fibrosis cases show distinct neutrophilic patterns.
Symptoms of Nasal Polyps
Symptoms depend on polyp size and location. Small polyps often cause no issues, but growth leads to progressive obstruction. Common symptoms include:
- Persistent nasal congestion or stuffy nose
- Runny nose (rhinorrhea) or postnasal drip
- Reduced or loss of smell (anosmia) and taste
- Facial pressure or pain
- Snoring and sleep disturbances
- Frequent sinus infections
Large or clustered polyps mimic chronic sinusitis, causing headaches, fatigue, and mouth breathing. Complications may include obstructive sleep apnea, mucocele formation (cysts leading to vision issues or eye bulging), or permanent anosmia.
Causes and Risk Factors
The exact cause remains unclear, but chronic inflammation is central—why some develop polyps while others with inflammation do not is unknown. Key triggers include:
- Chronic rhinosinusitis (CRS): Primary association, with polyps as an end-stage of uncontrolled inflammation.
- Asthma and allergies: Especially allergic rhinitis; familial risk shows 4.1-fold increase in first-degree relatives.
- Aspirin sensitivity (AERD): Triad of polyps, asthma, and aspirin intolerance.
- Cystic fibrosis: Common in young patients, especially European ancestry; neutrophilic polyps without allergies.
- Other: Allergic fungal sinusitis, eosinophilic granulomatosis (Churg-Strauss), immune defects allowing bacterial biofilms.
Risk factors heighten with age, though prevalent in adults 30-60; men slightly more affected.
How Are Nasal Polyps Diagnosed?
Diagnosis begins with history of persistent symptoms (>12 weeks) and physical exam using nasal endoscopy—a thin, flexible tube with camera to visualize polyps as pale, movable masses in middle meatus. Imaging like CT scans assesses extent, sinus involvement, or complications (e.g., mucoceles); MRI for soft tissue detail if needed. No biopsy unless malignancy suspected (rare). Differential includes tumors, antrochoanal polyps, or fungal balls. Associated conditions like asthma or CF tested via sweat chloride or genetic screening.
Nasal Polyps Treatment
Treatment targets inflammation and underlying causes; polyps rarely resolve spontaneously. Options:
- Medical therapy (first-line):
- Intranasal corticosteroids (e.g., fluticasone, budesonide): Shrink polyps, reduce congestion; 2-3 months trial.
- Saline irrigations: High-volume rinses clear mucus, allergens, biofilms.
- Oral corticosteroids: Short courses for severe cases.
- Biologics: Dupilumab (IL-4/13 inhibitor), omalizumab (anti-IgE), mepolizumab (anti-IL-5) for refractory CRSwNP.
- Antibiotics: For bacterial superinfections; macrolides (e.g., doxycycline) have anti-inflammatory effects.
- Avoid triggers: Aspirin desensitization for AERD; allergy management.
Medications control but don’t eliminate polyps; recurrence common without maintenance.
Surgery for Nasal Polyps
Indicated if medical therapy fails after 12 weeks or severe obstruction. Endoscopic sinus surgery (ESS) or polypectomy uses microscopes/instruments via nose under anesthesia to remove polyps and open sinuses. Minimally invasive, outpatient; improves airflow, smell. Recurrence risk 40-90% in 4 years without meds; post-op intranasal steroids/saline essential. Aspirin triad patients higher recurrence.
| Treatment | Pros | Cons |
|---|---|---|
| Intranasal Steroids | Non-invasive, effective shrinkage | Daily use, slow onset |
| Biologics | Targets inflammation, fewer side effects | Costly, injections |
| Endoscopic Surgery | Rapid symptom relief | Recurrence risk, anesthesia |
Prevention and Management
Prevent recurrence by controlling inflammation:
- Daily saline rinses and nasal steroids.
- Treat asthma/allergies per guidelines.
- Avoid irritants (smoke, pollutants).
- Humidify air; stay hydrated.
- Monitor with regular ENT follow-ups.
Lifestyle aids mucus flow, reduces triggers.
When to See a Doctor
Seek care for persistent (>12 weeks) congestion, smell loss, recurrent infections, facial pain, or breathing issues. Urgent if vision changes, severe headache, or swelling—may signal complications. ENT specialists manage; primary care for initial eval.
Frequently Asked Questions (FAQs)
Are nasal polyps cancerous?
No, nasal polyps are benign. Cancer risk low (<1%); suspicious features prompt biopsy.
Do nasal polyps go away on their own?
Rarely; chronic inflammation persists without treatment. Meds shrink, surgery removes.
How long do nasal polyps last?
Indefinitely without intervention; recurrence post-treatment possible in years.
Can nasal polyps affect sleep?
Yes, via obstruction causing snoring, apnea, fatigue.
Who is at risk for nasal polyps?
Those with CRS, asthma, allergies, CF, aspirin sensitivity; adults 30-60.
Content medically reviewed for accuracy using peer-reviewed sources. Consult healthcare provider for personalized advice.
References
- Nasal Polyps – StatPearls — NCBI Bookshelf/NCBI. 2023. https://www.ncbi.nlm.nih.gov/books/NBK560746/
- Nasal polyps: Symptoms, causes, treatment, and more — Medical News Today. 2023-10-24. https://www.medicalnewstoday.com/articles/177020
- Nasal Polyps: Symptoms, Causes, Treatment & Removal — Cleveland Clinic. 2023-05-10. https://my.clevelandclinic.org/health/diseases/15250-nasal-polyps
Similar Articles






Read full bio of Sneha Tete