Palmoplantar Pustulosis: Clinical Features & Management
Comprehensive guide to palmoplantar pustulosis: symptoms, causes, diagnosis, and evidence-based treatment strategies.

Understanding Palmoplantar Pustulosis
Palmoplantar pustulosis (PPP) is a benign, chronic, and often relapsing sterile pustular dermatosis that affects the palms and soles. This condition is characterized by recurrent eruptions of small to large sterile blisters filled with a yellow turbid liquid, known as pustules, appearing on the palms of the hands and/or soles of the feet. The disease is debilitating and often resistant to treatment, typically persisting for years with periods of partial or total remission interrupted by recurrent exacerbations. While palmoplantar pustulosis can be classified as a variant of psoriasis or as a separate entity, it represents one of the more challenging areas to treat in dermatology due to its location and chronic nature.
Clinical Presentation and Appearance
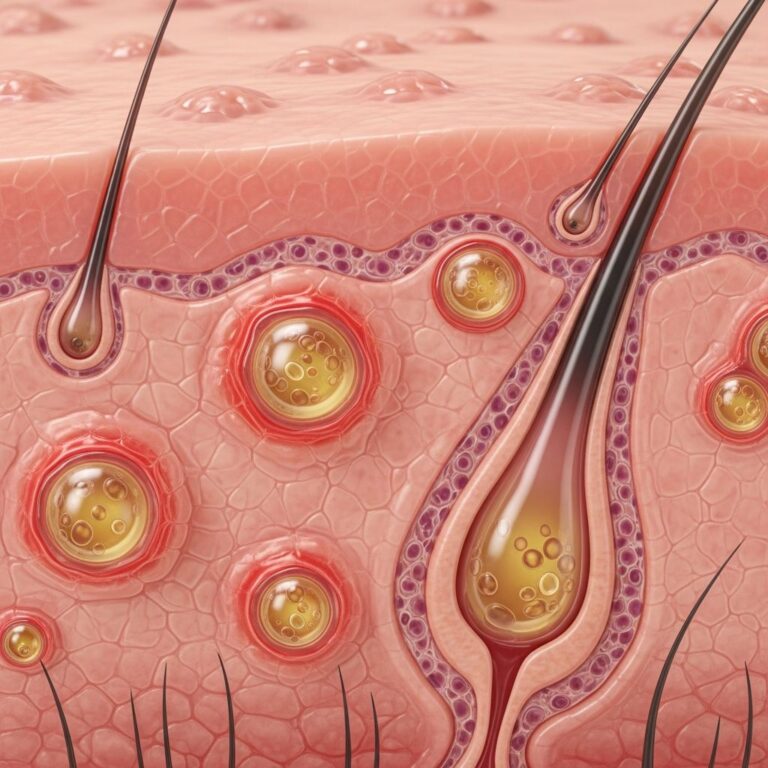
PPP manifests clinically as sterile, erupting pustules located on the palms and soles, occurring on a desquamative and erythematous background. The lesions are usually symmetrical and develop in abundant eccrine sweat gland affluent areas, which probably play a role in the pathogenesis of the condition. Pustules are more commonly noted on the thenar and hypothenar eminences and central palm, as well as the instep, medial and lateral borders of the foot, and the sides or back of the heel.
In flare-ups, the skin appears red, with tiny blisters filled with yellow or white liquid (pustules) that eventually turn brown and become scaly. The pustules often merge on a red, inflamed background, and over several days, these pustules can form scaly plaques with painful cracks.
Key Symptoms and Signs
Patients with palmoplantar pustulosis typically experience the following symptoms:
- Recurrent crops of sterile pustules on the palms and/or soles
- Pustules that merge on a red, inflamed background
- Formation of scaly plaques with painful cracks over several days
- Itching sensation
- Burning sensation in affected areas (often more common than itching)
- Pain and discomfort
- Difficulty walking and performing daily tasks due to symptoms affecting hands and feet
- Possible psoriatic nail changes
Patients complain of varying levels of pruritus; however, a more common complaint is of a burning sensation. Lesions may also develop into painful fissures, significantly impacting quality of life and daily functioning.
Epidemiology and Risk Factors
Palmoplantar pustulosis primarily affects females between 40 and 69 years of age, and it predominantly occurs in smokers. The majority of patients with PPP are cigarette smokers, with 70-90% of patients being current or former smokers. This strong association with smoking is one of the most distinctive features of the condition.
Etiology and Triggering Factors
The exact cause of PPP is not known; however, researchers have determined that a combination of genetics, autoinflammatory, and environmental factors likely play a role in its development. Several specific triggering factors have been identified:
Smoking
Smoking is the most prominent risk factor and disease-aggravating factor in PPP. It is thought that activated nicotine receptors in the sweat glands stimulate an inflammatory process. An estimated 65-90% of patients with PPP smoke or have smoked in the past. Smoking may cause sweat glands to become inflamed, especially on the hands and feet, which causes pustules to form.
Infections
Infections represent a well-recognized triggering factor in palmoplantar pustulosis. Many case reports describe an association between PPP and specific bacterial infections, including:
- Tonsillitis and recurrent upper respiratory infections
- Odontogenic infection (dental infection) — the most commonly reported
- Chronic sinusitis
- Chlamydia trachomatis infections
- Helicobacter pylori (based on anecdotal case reports)
Clinical improvement in more than half of patients with PPP has been observed by controlling dental disease. The association between infections and PPP might be explained by an immune reaction to outside antigens that promotes autoreactivity features in individuals already genetically predisposed.
Genetic Factors
Genetics may play a role in PPP development, with some patients having a family history of the disorder. Research has identified a mutation in the gene IL36RN appearing in around 5% of PPP patients, supporting the genetic component of the disease. Furthermore, a family history of psoriasis has been reported in 10-42% of people with PPP.
Additional Triggering Factors
Other factors associated with PPP onset and exacerbation include:
- Contact allergies: Patients with PPP may be allergic to nickel, chromium, mercury, and fragrances. Withdrawal of the metal allergen may improve PPP symptoms.
- Medications: Biological therapies, mainly anti-TNF-alpha molecules used to treat chronic inflammatory conditions, have been associated with PPP onset due to activation of the innate immune system.
- Stress: Emotional stress may exacerbate symptoms.
- Hormonal changes: Fluctuations in hormone levels may trigger or worsen the condition.
- Environmental factors: Exposure to irritants and allergens can trigger flare-ups.
Relationship to Psoriasis
PPP is strongly related to psoriasis vulgaris. Some patients have both PPP and plaque psoriasis or PPP and psoriatic arthritis. Psoriatic nail involvement is frequently seen in PPP. This overlap has led to ongoing debate about whether PPP should be considered a variant of psoriasis or a separate entity, though it is often classified as localised pustular psoriasis in dermatological practice.
Pathophysiology
The pathogenesis of PPP is still poorly understood; however, research has provided insights into the inflammatory mechanisms involved. In the skin of PPP, the inflammatory process affects the intraepidermal duct of the eccrine ducts or acrosyringium, leading to their elimination. Studies have shown that in affected skin, there is a reduction in the number of acrosyringeal ducts, and research has validated that the development of pustules begins in the acrosyringium. This connection to sweat gland pathology helps explain why the condition primarily affects the palms and soles, which have abundant eccrine sweat glands.
Diagnosis
Diagnosis of palmoplantar pustulosis is primarily clinical, based on the characteristic presentation of sterile pustules on the palms and soles with an erythematous and scaly background. The diagnosis typically involves:
- Clinical examination of affected areas
- Assessment of lesion distribution and morphology
- Patient history regarding smoking, infections, and symptom onset
- Evaluation of nail changes if present
- Patch testing if contact dermatitis is suspected
A distinguishing feature is that the pustules are sterile—meaning they do not contain bacteria and are not infectious. This differentiates PPP from pustular infections and supports the diagnosis of an inflammatory dermatological condition rather than an infectious process.
Treatment Approach
There is no cure for palmoplantar pustulosis, and its treatment is challenging, as currently there is no approved treatment specifically for this disease. However, depending on the cause and severity, many treatments are available. The treatment approach involves both topical and systemic therapies, as well as phototherapy and targeted molecules. No gold standard therapy has yet been identified, and none of the treatments are curative.
First-Line Topical Therapies
Treatment typically starts with topical therapies applied directly to the affected areas:
- Topical Steroids: Applied directly to blisters to reduce inflammation
- Vitamin D Derivatives: Help reduce the severity of lesions
- Emollients (Moisturizers): Keep the skin soft and reduce cracking
- Occlusion: In patients with mild disease, control may be achieved with on-demand occlusion of topical agents
Phototherapy
Phototherapy involves exposing the skin to certain types of light and includes several effective options:
- UVA and UVB Therapies: Help reduce symptoms with minimal side effects
- Excimer Laser: Effective, especially at higher doses
- PUVA Therapy: Combines a drug called psoralen with UVA light; very effective, especially for the palms
Systemic Therapies
If initial treatments do not provide adequate control, systemic therapies may be prescribed:
- Retinoids: Can be prescribed if topical therapies and phototherapy prove insufficient
- Ciclosporin: A fast-acting medication used for severe cases, but symptoms may return quickly after stopping treatment
- Methotrexate: Another option for severe cases; helps by suppressing the immune system
Advanced Treatments
For severe cases resistant to conventional therapies, biologic medications offer newer options that target specific parts of the immune system. Biologics tend to work better over longer periods. Additionally, JAK inhibitors represent a potential future option, pending more research.
Lifestyle and Preventive Measures
Comprehensive management also involves lifestyle modifications and preventive strategies:
- Quitting Smoking: Since PPP is common in smokers, smoking cessation can help improve symptoms significantly
- Avoiding Irritants: Protecting the hands and feet by avoiding contact with irritants such as wet work, aggressive soaps, and detergents; using gloves when necessary
- Managing Infections: Prompt treatment of bacterial infections, particularly dental infections, tonsillitis, and respiratory infections
- Reducing Stress: Limiting stress may help improve symptoms
- Avoiding Contact Allergens: Identifying and eliminating exposure to metal allergens (nickel, chromium) or other contact sensitizers
Treatment Algorithm
In summary, treatment typically follows a stepwise approach:
- Begin with topical therapies and phototherapy
- If initial treatments are inadequate, prescribe retinoids
- If retinoids cause side effects or prove ineffective, consider ciclosporin or methotrexate
- For severe cases unresponsive to other options, utilize biologic therapies
- Monitor for emerging JAK inhibitor therapies as potential future options
The choice of treatment depends on disease severity, patient preferences, comorbidities, and response to previous therapies.
Frequently Asked Questions (FAQs)
Q: Is palmoplantar pustulosis contagious?
A: No, palmoplantar pustulosis is not contagious. The pustules are sterile, meaning they do not contain bacteria and are not infectious. PPP is an inflammatory skin condition, not an infection.
Q: Can palmoplantar pustulosis be cured?
A: There is currently no cure for palmoplantar pustulosis. However, various treatments can effectively manage symptoms and help achieve periods of remission. Treatment focuses on controlling flare-ups and improving quality of life.
Q: How does smoking affect palmoplantar pustulosis?
A: Smoking is a major risk factor and disease-aggravating factor in PPP. It is believed that activated nicotine receptors in sweat glands stimulate inflammatory processes. Quitting smoking can significantly improve symptoms in many patients.
Q: What is the relationship between palmoplantar pustulosis and psoriasis?
A: PPP is strongly related to psoriasis vulgaris and is sometimes classified as a variant of psoriasis (localized pustular psoriasis). Some patients have both PPP and plaque psoriasis. However, whether PPP is truly a psoriasis variant or a separate entity remains debated among dermatologists.
Q: Can dental infections cause palmoplantar pustulosis?
A: Yes, odontogenic (dental) infections have been frequently associated with PPP. Clinical improvement has been observed in more than half of patients when dental disease is properly treated or controlled, making dental health important in PPP management.
Q: What should I avoid if I have palmoplantar pustulosis?
A: Patients with PPP should avoid wet work, aggressive soaps and detergents, contact allergens (particularly nickel and chromium), excessive stress, smoking, and irritants to the hands and feet. Protective measures such as wearing gloves during household tasks can help prevent exacerbations.
Q: How long does palmoplantar pustulosis typically last?
A: PPP is a chronic condition that typically persists for years with periods of partial or total remission interrupted by recurrent exacerbations. The duration and severity of flare-ups vary among individuals and depend on triggers and treatment effectiveness.
References
- Palmoplantar Pustulosis – Symptoms, Causes, Treatment — National Organization for Rare Disorders (NORD). Accessed 2025. https://rarediseases.org/rare-diseases/palmoplantar-pustulosis/
- Diagnosis, Screening and Treatment of Patients with Palmoplantar Pustulosis — PubMed Central, National Center for Biotechnology Information. 2020. https://pmc.ncbi.nlm.nih.gov/articles/PMC7439281/
- Palmoplantar pustulosis — Almirall. Accessed 2025. https://www.almirall.com/your-health/your-skin/skin-conditions/rare-skin-diseases/palmoplantar-pustulosis
- Psoriasis diagnosis and treatment. Palmoplantar Pustulosis — Levit Dermatology, YouTube. July 16, 2024. https://www.youtube.com/watch?v=Xk_dE1wfMW4
- Palmoplantar Pustulosis (localised pustular psoriasis) — DermNet. Accessed 2025. https://dermnetnz.org/topics/palmoplantar-pustulosis
- Palmoplantar pustulosis — BAD Patient Hub – Skin Health Info. Accessed 2025. https://www.skinhealthinfo.org.uk/condition/palmoplantar-pustulosis/
Similar Articles






Read full bio of Sneha Tete