Peripapillary Atrophy: A Clear Guide For Diagnosis And Care
Discover what peripapillary atrophy means for your eye health, its links to myopia and glaucoma, and why regular exams matter.

Peripapillary atrophy refers to the thinning and degeneration of tissues encircling the optic nerve head in the retina. This condition alters the normally vibrant pink hue of the peripapillary region to pale white, yellowish, or dark shades, potentially signaling underlying eye issues.
The Optic Nerve and Its Surrounding Tissues
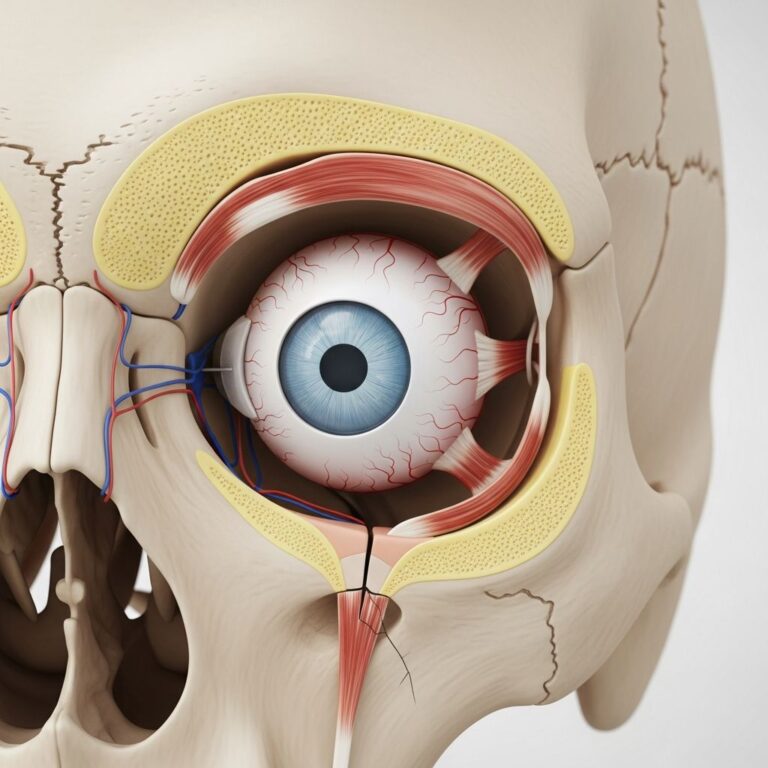
The optic nerve, often called the optic disc, serves as the vital conduit transmitting visual signals from the retina to the brain. Surrounding this disc is a layered structure including the retinal pigment epithelium (RPE), choroid, and sclera. In healthy eyes, these layers maintain a uniform pink appearance due to rich blood supply and pigmentation.
When peripapillary atrophy develops, these layers thin out, exposing underlying sclera or causing pigment loss. This creates visible crescents or rings around the disc, observable during fundus examinations. The change stems from stretching or degeneration, often benign but sometimes indicative of progressive pathology.
Types of Peripapillary Atrophy
Clinicians classify peripapillary atrophy into distinct zones based on proximity to the optic disc and histological features. The primary divisions are alpha and beta zones, with gamma zone noted in severe cases.
- Alpha Zone: Located farther from the disc, this outer region shows RPE irregularities without complete loss. It appears as mottled pigmentation and is common in normal eyes, especially myopic ones, without implying disease.
- Beta Zone: Adjacent to the disc, this inner area involves total RPE and photoreceptor loss, choroidal thinning, and scleral visibility. Present in 15-20% of healthy eyes, its enlargement correlates with glaucoma risk, optic nerve damage, and vision loss.
- Gamma Zone: Seen in extreme myopia, this extends beyond beta, exposing deeper sclera due to marked axial elongation.
These zones help differentiate benign findings from those warranting intervention. Location matters too: temporal atrophy is typical in myopia, while superior or inferior involvement raises glaucoma suspicion.
Primary Causes and Risk Factors
High myopia tops the list of causes, where elongated eyeballs stretch peripapillary tissues. Prescriptions beyond -7.00 diopters heighten risk, leading to mechanical stress on the optic nerve border.
Glaucoma represents a pathologic driver, where elevated intraocular pressure damages the optic nerve, enlarging beta-zone atrophy over time. Studies confirm larger beta zones in glaucomatous eyes, associating them with retinal nerve fiber layer thinning and field defects.
Other factors include aging, optic neuropathies, and chorioretinal disorders. Spectral domain optical coherence tomography (SD-OCT) reveals specifics like RPE disruption (82% of cases), photoreceptor loss (29%), and cystic changes.
| Risk Factor | Description | Prevalence Link |
|---|---|---|
| High Myopia | Axial elongation stretches tissues | Common in -7D+ prescriptions |
| Glaucoma | Pressure-induced damage | Enlarging beta zone |
| Aging | Natural degeneration | Increased alpha zone |
| Optic Neuropathy | Inflammatory/infectious causes | RPE irregularities |
Symptoms and Clinical Presentation
Most individuals experience no symptoms, earning it the label of an incidental finding during routine exams. The optic nerve’s appearance shifts abnormally—pale crescents replace healthy pigmentation—but central vision remains unaffected initially.
In progressive cases tied to glaucoma, subtle peripheral vision loss may emerge. Myopic patients might notice distorted peripheral views if atrophy advances. Unlike optic atrophy, which directly impairs nerve fibers and causes vision decline, peripapillary atrophy primarily alters structure without immediate functional loss.
Diagnosis Through Advanced Imaging
Detection occurs via dilated funduscopy, revealing color and contour changes. SD-OCT provides detailed cross-sections, quantifying atrophy extent and identifying features like RPE/photoreceptor loss, retinal thinning, and choroidal defects.
Key OCT hallmarks include:
- Hyper-reflective sclera with signal penetration into choroid.
- RNFL plaque-like thickening or cysts.
- Sloping retinal borders.
Progression monitoring involves serial imaging; expanding beta-zone area signals glaucoma, prompting pressure checks and visual fields.
Is Treatment Available?
No direct therapy exists for peripapillary atrophy itself, as it reflects structural change rather than reversible disease. Management targets underlying causes: myopia control via orthokeratology or atropine drops in youth; glaucoma with pressure-lowering drops, lasers, or surgery.
Annual dilated exams suffice for stable cases. High-risk patients (large/enlarging atrophy) require frequent monitoring to avert vision-threatening complications.
Peripapillary Atrophy in Myopia Versus Glaucoma
Myopia: Predominantly alpha/gamma zones temporally; stable, non-progressive. Beta zone, if present, is smaller.
Glaucoma: Beta zone dominates, often superior/inferior; grows over time, with RNFL defects and hemorrhages.
Differentiating relies on history, refraction, pressure, and imaging trends.
Prevention and Long-Term Eye Care
While not fully preventable, risks lessen through:
- Regular comprehensive exams, especially post-40 or with myopia.
- UV protection and healthy lifestyle to curb oxidative stress.
- Early myopia management in children.
Patient education emphasizes vigilance; many live asymptomatically lifelong.
Common Misconceptions
- It’s always glaucoma: No—most cases benign, myopia-related.
- Vision loss is immediate: Rarely; progression is key concern.
- No monitoring needed: Incorrect—annual checks essential.
Frequently Asked Questions (FAQs)
What exactly causes the color change in peripapillary atrophy?
Thinning exposes white sclera or loses pigmented RPE/choroid, shifting from pink to white/yellow/black.
Can peripapillary atrophy lead to blindness?
Not directly; associated glaucoma can if unmanaged.
How often should I get checked if diagnosed?
Annually or more if progressing/large.
Is it hereditary?
Myopia link suggests partial genetic role; glaucoma multifactorial.
Does laser surgery fix it?
No—targets glaucoma pressure, not atrophy.
Latest Research Insights
Recent SD-OCT studies (post-2020) refine beta-zone metrics as glaucoma predictors, with AI enhancing detection. Longitudinal data affirm progression links to axial length and pressure.
References
- Peripapillary Atrophy – CorneaCare — MyCorneaCare. 2023. https://mycorneacare.com/glossary/peripapillary-atrophy/
- What is Peripapillary Atrophy and How is it Treated? — West Boca Eye Center. 2023. https://www.westbocaeyecenter.com/post/what-is-peripapillary-atrophy-and-how-is-it-treated
- Analysis of Peripapillary Atrophy using Spectral Domain Optical… — PMC (NCBI). 2011-02-01. https://pmc.ncbi.nlm.nih.gov/articles/PMC3017221/
- Optic Atrophy: Causes, Symptoms & Treatment — Cleveland Clinic. 2023. https://my.clevelandclinic.org/health/diseases/12326-optic-atrophy
- Peripapillary Atrophy Area as an Indicator of Glaucomatous… — ARVO Journals (TVST). 2023. https://tvst.arvojournals.org/article.aspx?articleid=2793419
Similar Articles






Read full bio of Sneha Tete