Purpura: Causes, Symptoms, Diagnosis & Treatment Guide
Comprehensive guide to purpura: causes, types, symptoms, diagnosis, and treatment options for this common skin haemorrhage condition.

What is purpura?
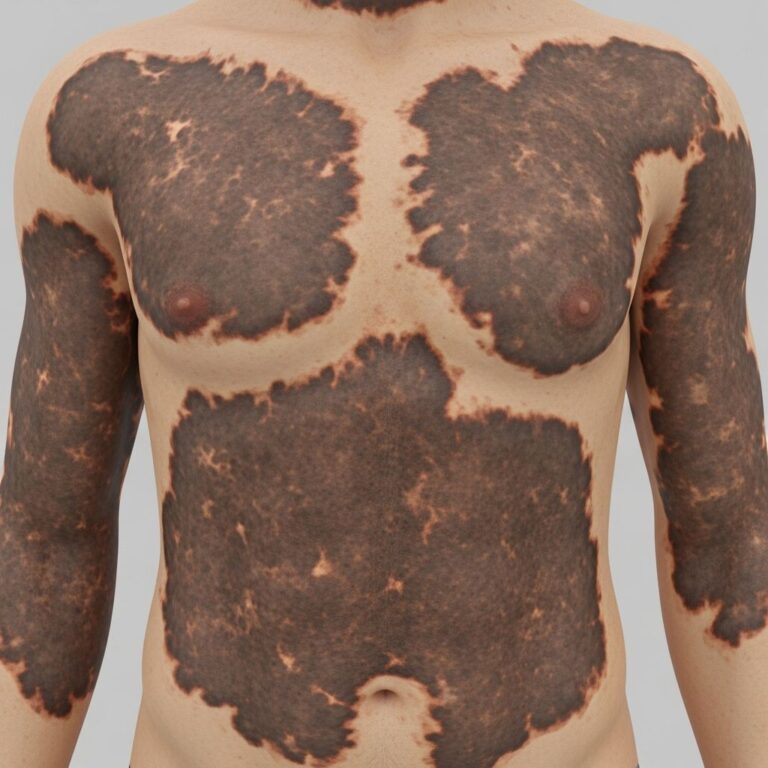
Purpura refers to the discolouration of the skin or mucous membranes resulting from haemorrhage beneath the epidermis due to extravasation of blood from small vessels. These lesions are non-blanching, meaning they do not fade under pressure, distinguishing them from other rashes like erythema. Purpura spots typically measure 4–10 mm in diameter, appearing as small purple, red, or brown spots caused by blood pooling under the skin when tiny vessels burst. Unlike petechiae (<4 mm), purpura lesions are larger, while ecchymoses exceed 1 cm. This condition can signal minor trauma or serious disorders like clotting issues or infections.
The term encompasses a spectrum from tiny petechiae to extensive ecchymoses, often appearing on the limbs, mucous membranes, or trunk. On lighter skin, they present as purple-red; on darker tones, they may look darker brown or black. Purpura arises from vessel fragility, low platelets, or coagulation defects, requiring identification of the underlying cause for proper management.
Who gets purpura?
Purpura affects individuals across all ages, with prevalence varying by type. Thrombocytopenic purpura is common in children with immune thrombocytopenia (ITP) and adults on certain medications or with infections. Elderly patients frequently develop senile purpura due to fragile skin and vessels from photoageing and corticosteroid use.
- Children: Often IgA vasculitis (Henoch-Sch f6nlein purpura), infections, or ITP.
- Adults: Medications, malignancies, autoimmune diseases, or amyloidosis.
- Elderly: Senile or actinic purpura from dermal thinning and capillary fragility.
- Immunocompromised: Higher risk from HIV, chemotherapy, or transplants.
Risk factors include advanced age, poor nutrition (e.g., vitamin C deficiency causing scurvy), connective tissue disorders like Ehlers-Danlos syndrome, and chronic sun exposure. Women may experience it during pregnancy or with hormone therapies.
What causes purpura?
Purpura results from three main mechanisms: platelet disorders (thrombocytopenia), coagulation defects, or vascular fragility (non-thrombocytopenic). Treatment targets the root cause.
Thrombocytopenic purpura
Occurs when platelet counts drop below 100,000/μL, impairing clot formation. Platelets are destroyed or production fails.
| Causes | Examples |
|---|---|
| Immune-mediated | Idiopathic thrombocytopenic purpura (ITP), drug-induced, HIV |
| Infections | Hepatitis C, EBV, CMV, Rocky Mountain spotted fever |
| Malignancies | Leukaemia, lymphoma affecting bone marrow |
| Medications/Treatments | Chemotherapy, heparin, oestrogens |
In ITP, autoantibodies attack platelets, common post-viral in children.
Coagulation disorders
Impaired clotting factors lead to widespread bleeding.
- Haemophilia, von Willebrand disease.
- Disseminated intravascular coagulation (DIC) from sepsis or trauma.
- Vitamin K deficiency or warfarin overdose.
Vascular causes (non-thrombocytopenic purpura)
Blood leaks through intact vessel walls due to fragility.
| Category | Specific Causes |
|---|---|
| Congenital | Ehlers-Danlos syndrome, Marfan syndrome, hereditary haemorrhagic telangiectasia |
| Acquired | Senile purpura, actinic purpura, scurvy (vitamin C deficiency), amyloidosis |
| Inflammatory | Henoch-Sch f6nlein purpura (IgA vasculitis), cryoglobulinaemia |
| Infections | Meningococcaemia, endocarditis |
| Drugs | Steroids, NSAIDs causing vessel fragility |
Senile purpura affects forearms in the elderly from solar elastosis weakening vessel supports. Henoch-Sch f6nlein purpura inflames small vessels, often post-infection in kids.
What are the signs and symptoms of purpura?
Signs vary by type but include non-blanching purple-red macules or patches.
- Thrombocytopenic: Widespread petechiae on legs, gums bleeding, easy bruising, epistaxis.
- Non-thrombocytopenic: Localised crops on legs/arms, palpable in vasculitis.
- Senile: Large ecchymoses on forearms/back of hands, resolving slowly.
Associated symptoms: fever, arthralgia, abdominal pain (in HSP), fatigue, haematuria. Seek urgent care for mucosal bleeding, joint swelling, or neurological signs indicating severe thrombocytopenia or infection.
How is purpura diagnosed?
Diagnosis combines history, exam, and tests to pinpoint mechanism.
- Clinical exam: Non-blanching lesions >4 mm; distribution/pattern clues (e.g., legs in HSP).
- Blood tests: FBC (platelets), coagulation profile, renal function.
- Specific: ANA for lupus, ASOT for streptococcal trigger, bone marrow biopsy if needed.
- Skin biopsy: For vasculitis confirmation (leucocytoclastic changes).
Platelet count <20,000/μL suggests severe risk; normal levels point to vascular causes.
What is the treatment for purpura?
Treat underlying cause; supportive for mild cases.
- Thrombocytopenic: Steroids (prednisolone 1 mg/kg), IVIG for ITP; platelet transfusions if <10,000/μL or bleeding. Rituximab for refractory cases.
- Vasculitis (HSP): Supportive; steroids for severe abdominal/renal involvement.
- Senile: Protection from trauma, vitamin C, arnica. Avoid aspirin/NSAIDs.
- Infections: Antibiotics for meningococcaemia.
Monitor for complications like renal failure in HSP.
What is the outcome for purpura?
Prognosis depends on cause. Benign senile purpura recurs but harmless; ITP often remits in children (80% spontaneous). Serious cases like TTP or DIC have high mortality without prompt treatment. HSP resolves in weeks but 1–5% develop chronic nephritis. Early intervention improves outcomes.
Related topics
- Petechiae
- Ecchymoses
- Henoch-Sch f6nlein purpura
- Idiopathic thrombocytopenic purpura
- Senile purpura
- Vasculitis
Frequently Asked Questions
Q: Is purpura dangerous?
A: Most cases are benign, but widespread or mucosal purpura with low platelets requires urgent evaluation for bleeding risks or serious disease.
Q: Does purpura blanch on pressure?
A: No, purpura is non-blanching, unlike erythema; use glass test to confirm.
Q: Can purpura be caused by medications?
A: Yes, drugs like steroids, chemotherapy, or anticoagulants commonly cause it via platelet reduction or vessel fragility.
Q: How long does purpura last?
A: Simple lesions fade in 1–2 weeks; underlying disease may prolong or recur.
Q: When to see a doctor for purpura?
A: Immediately if accompanied by fever, bleeding, joint pain, or in children/elderly.
References
- Purpura: Causes, pictures, and symptoms — Medical News Today. 2023-05-12. https://www.medicalnewstoday.com/articles/311725
- Purpura: Causes, Types and Images — DermNet NZ. 2024-01-15. https://dermnetnz.org/topics/purpura
- Purpura: Causes, Symptoms, and Treatment — Healthgrades. 2024-08-20. https://resources.healthgrades.com/right-care/skin-hair-and-nails/purpura
- Purpura: Causes, Diagnosis, Treatment, and Pictures — Healthline. 2023-11-05. https://www.healthline.com/health/purpura
- Purpura — MedlinePlus, U.S. National Library of Medicine. 2025-02-10. https://medlineplus.gov/ency/article/003232.htm
- Henoch-Schonlein purpura – Symptoms & causes — Mayo Clinic. 2024-06-18. https://www.mayoclinic.org/diseases-conditions/henoch-schonlein-purpura/symptoms-causes/syc-20354040
Similar Articles






Read full bio of medha deb