Radiation Dermatitis: Symptoms, Prevention, Treatment Guide
Comprehensive guide to radiation-induced skin reactions: causes, symptoms, grades, management, and prevention strategies for patients undergoing radiotherapy.

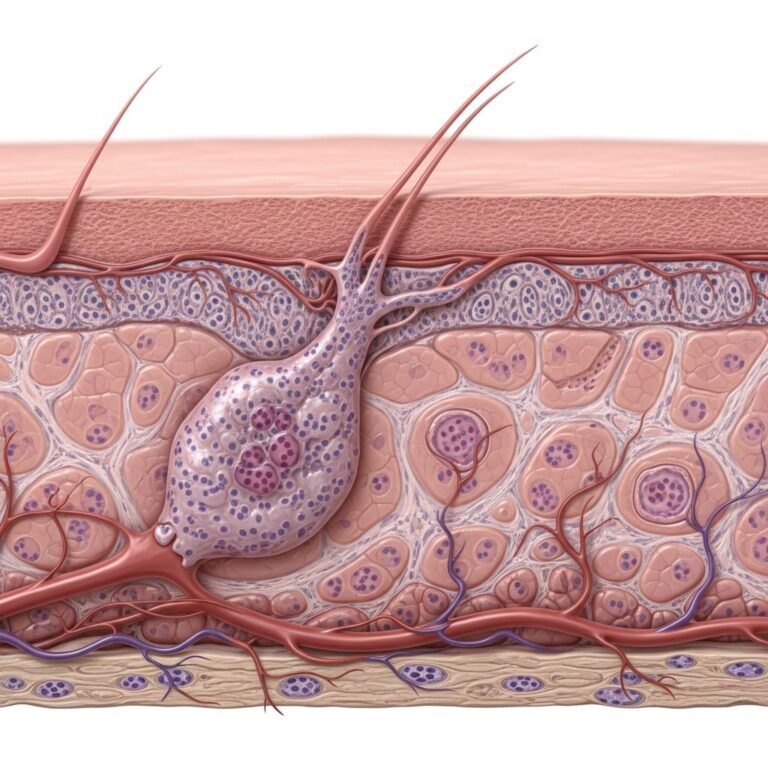
Radiation dermatitis, also known as radiodermatitis, is an inflammatory skin reaction triggered primarily by radiotherapy for cancer treatment. It affects nearly all patients receiving radiation therapy, manifesting as damage to the skin’s epidermal and dermal layers due to ionizing radiation exposure.
What is Radiation Dermatitis?
Radiation dermatitis refers to a range of cutaneous reactions resulting from exposure to ionizing radiation, most commonly during therapeutic radiotherapy for malignancies such as breast, head and neck, or skin cancers. Less frequently, it arises from accidental overexposure or interventional radiology procedures like angiography. The condition arises when radiation penetrates the skin to target underlying tumors, inevitably damaging healthy skin cells in the process.
The skin reaction is sharply confined to irradiated areas, appearing days to weeks after treatment initiation, depending on dose, fractionation, and individual sensitivity. Acute forms develop within 90 days, while chronic effects may persist or emerge years later.
Who Gets Radiation Dermatitis?
Up to 95% of radiotherapy patients experience some degree of radiation-induced dermatitis (RID), with severity varying by treatment site and protocol. It is most prevalent in those receiving external beam radiation for breast cancer (common due to chest wall exposure), head and neck cancers, or superficial tumors like skin or anal cancers.
Risk is heightened in patients with pre-existing skin conditions, genetic predispositions, or treatments involving high doses over large areas.
Acute Radiation Dermatitis
Acute radiation dermatitis occurs within weeks of starting radiotherapy and typically resolves post-treatment, though healing can take months. It stems from direct radiation damage to basal keratinocytes, endothelial cells, and inflammatory cascades generating reactive oxygen species.
Clinical Features
Symptoms begin subtly and escalate:
- Early erythema: Faint redness within 24 hours, resolving quickly.
- Main phase (weeks 2-4): Sustained erythema, dry desquamation (peeling), dryness, pruritus, pain, edema, and hyperpigmentation.
- Severe cases: Moist desquamation (weeping skin), blistering, ulceration, and secondary infection risk.
Skin may appear sunburn-like, with itching, swelling, or blotchy discoloration (darker on skin of color).
Grading of Acute Radiation Dermatitis
Severity is graded using systems like the Common Terminology Criteria for Adverse Events (CTCAE):
| Grade | Symptoms |
|---|---|
| 1 (Mild) | Faint erythema, dry peeling. |
| 2 (Moderate) | Moderate erythema, patchy moist desquamation (skin folds), edema. |
| 3 (Severe) | Moist desquamation >1.5 cm, pitting edema, ulceration. |
| 4 (Life-threatening) | Necrosis, skin ulceration, bleeding. |
Higher grades may necessitate treatment interruptions, impacting cancer outcomes.
Chronic Radiation Dermatitis
Chronic radiation dermatitis develops months to years post-radiotherapy, resulting from persistent vascular damage, fibrosis, and telangiectasia. It features atrophy, induration, dyspigmentation, and increased skin cancer risk.
Key features include:
- Permanent telangiectasias and fibrosis.
- Fragile, atrophic skin prone to ulceration.
- Delayed ulcers or necrosis years later.
Management focuses on wound care and monitoring for malignancy.
Pathophysiology
Radiation induces free radical formation, depleting epidermal stem cells and damaging DNA in basal layers. This triggers cytokine release (e.g., IL-1, TNF-α, CXCL10, CCL2), leukocyte infiltration, and vascular endothelial changes, culminating in inflammation, edema, and barrier disruption.
Subsequent doses prevent repair, amplifying damage to sebaceous glands (dryness) and follicles (epilation).
Risk Factors
Several factors exacerbate RID:
- Treatment-related: High total dose (>50 Gy), large fields, hypofractionation, concurrent chemotherapy (e.g., taxanes).
- Patient-related: Fair skin, smoking, obesity, diabetes, prior sun damage.
- Site-specific: Breast, head/neck, perineum.
Prevention
Preventive strategies reduce severity:
- Skin hygiene: Daily mild soap washes, patting dry; avoid irritants.
- Moisturizers: Emollients like aqueous creams from day 1.
- Topical steroids: Low-potency (e.g., hydrocortisone) pre- and during treatment (not on open skin).
- Barrier films: Emerging evidence for silicone-based products.
- Avoid: Harsh soaps, alcohol wipes, tight clothing, sun exposure.
Treatment and Management
Treatment is supportive, tailored to grade:
- Grade 1-2: Moisturizers (petrolatum), topical steroids, oral analgesics.
- Grade 3+: Non-adherent dressings, silver sulfadiazine for infection, pain control; consider breaks.
- General care: Keep clean/dry, loose clothing, avoid swimming/pools.
Recent reviews endorse barrier creams and growth factor dressings for repair promotion.
Investigations
Diagnosis is clinical, based on history and irradiated-site confinement. Swabs rule out infection; biopsy rarely needed unless chronic or suspicious for malignancy.
Complications
- Secondary bacterial/fungal infections.
- Treatment delays reducing efficacy.
- Chronic fibrosis/ulceration, squamous cell carcinoma risk.
Patient Care and Advice
Patients should:
- Use fragrance-free emollients 2-3x daily.
- Protect from sun, trauma, heat.
- Report fever, pus, worsening pain promptly.
Frequently Asked Questions (FAQs)
Q: How common is radiation dermatitis?
A: Nearly all (95%) radiotherapy patients develop it to some degree.
Q: When does it start and resolve?
A: Symptoms appear 1-4 weeks into treatment; acute effects resolve 2-4 weeks post-therapy.
Q: Can it be prevented?
A: Not entirely, but skin care routines like moisturizing and hygiene significantly reduce severity.
Q: Is it painful?
A: Yes, especially grades 2-4, with burning, itching, and soreness; managed with topicals and analgesics.
Q: Does it increase cancer risk?
A: Chronic changes raise skin cancer risk in irradiated fields; regular follow-up advised.
References
- Radiation dermatitis: Symptoms, treatment, and prevention — Medical News Today. 2019-06-10. https://www.medicalnewstoday.com/articles/323155
- Radiation Burn (Dermatitis): Symptoms & Treatment — Cleveland Clinic. 2023-08-21. https://my.clevelandclinic.org/health/diseases/21995-radiation-burns
- Topical treatment of radiation-induced dermatitis — PubMed Central (PMC). 2020-06-19. https://pmc.ncbi.nlm.nih.gov/articles/PMC7295106/
- Radiation Dermatitis — Palliative Care Network of Wisconsin (mypcnow.org). 2023. https://www.mypcnow.org/fast-fact/radiation-dermatitis/
- Radiation dermatitis — DermNet NZ. 2023. https://dermnetnz.org/topics/radiation-dermatitis
- Radiation Therapy Side Effects — American Cancer Society. 2024-01-15. https://www.cancer.org/cancer/managing-cancer/treatment-types/radiation/effects-on-different-parts-of-body.html
- Skin Management – Radiation Therapy Algorithm — MD Anderson Cancer Center. 2022. https://www.mdanderson.org/content/dam/mdanderson/documents/for-physicians/algorithms/clinical-management/clin-management-skin-management-radiation-therapy-web-algorithm.pdf
Similar Articles






Read full bio of Sneha Tete