Resistant Hypertension: Understanding and Managing Treatment-Resistant High Blood Pressure
Learn about resistant hypertension, its causes, diagnostic evaluation, and advanced treatment options.

Understanding Resistant Hypertension
Resistant hypertension is a serious medical condition characterized by blood pressure that remains elevated despite the use of adequate doses of at least three different antihypertensive medications, typically including a diuretic. This condition affects a significant portion of the hypertensive population and requires specialized evaluation and management to prevent serious cardiovascular complications.
Unlike standard hypertension that responds well to lifestyle modifications and medication, resistant hypertension persists despite appropriate treatment adherence and medication optimization. Understanding this condition is essential for both patients and healthcare providers, as it often indicates an underlying medical problem that requires further investigation and targeted intervention.
Definition and Diagnostic Criteria
The medical definition of resistant hypertension has evolved over time as clinicians have gained better understanding of blood pressure control. Resistant hypertension is formally defined as the failure to achieve goal blood pressure despite adherence to maximum tolerated doses of three antihypertensive medications of different classes, typically including a diuretic.
Before confirming a diagnosis of resistant hypertension, healthcare providers must first exclude pseudoresistance, which includes conditions such as poor medication adherence and white coat hypertension (elevated blood pressure readings only in clinical settings). This distinction is critical because addressing pseudoresistance often resolves the apparent treatment resistance without requiring intensive additional therapy.
Risk Factors and Predisposing Conditions
Resistant hypertension is almost always multifactorial in etiology, meaning multiple factors contribute to its development. Several demographic and clinical factors increase the risk of developing treatment-resistant high blood pressure:
Demographic Risk Factors:
– Older age- Female sex- Black race- Residence in southeastern United States
Clinical and Lifestyle Risk Factors:
– Obesity- Excessive dietary salt ingestion- Chronic kidney disease- Diabetes mellitus- Left ventricular hypertrophy- High baseline blood pressure
Chronic kidney disease deserves special attention as a risk factor for resistant hypertension. Studies have shown that less than 15% of patients with chronic kidney disease achieve adequate blood pressure control despite using an average of three different antihypertensive agents. Treatment resistance in these patients is largely attributed to increased sodium and fluid retention, leading to intravascular volume expansion.
Common Causes of Resistant Hypertension
Understanding the underlying causes of resistant hypertension is fundamental to effective treatment. These causes can be broadly categorized into three main groups: lifestyle factors, medication-related factors, and secondary medical conditions.
Lifestyle and Behavioral Factors
Modifiable lifestyle factors play a substantial role in contributing to resistant hypertension. Common lifestyle factors include excessive alcohol consumption, obesity, poor dietary adherence (particularly high sodium intake), inadequate physical activity, and untreated obstructive sleep apnea. These factors often work synergistically to undermine the effectiveness of antihypertensive medications and must be addressed comprehensively as part of any treatment plan.
Medication-Related Causes
Numerous medications can interfere with blood pressure control or directly elevate blood pressure. These include both prescription and over-the-counter medications such as nonsteroidal anti-inflammatory drugs, sympathomimetic agents, oral contraceptives, corticosteroids, and immunosuppressive drugs. Additionally, poor medication adherence accounts for approximately 40% of resistant hypertension cases, as medications must be taken daily at the correct dose and frequency to be effective.
Secondary Causes of Hypertension
Secondary hypertension, caused by an identifiable underlying medical condition, often presents as resistant hypertension. Common secondary causes include hormonal abnormalities affecting blood pressure regulation, renal artery stenosis (narrowing of arteries leading to the kidneys), obstructive sleep apnea, and renal parenchymal disease. Identifying and treating these underlying conditions is crucial for achieving adequate blood pressure control.
Diagnostic Evaluation
Proper diagnostic evaluation is essential for identifying the cause of resistant hypertension and determining the most appropriate treatment strategy. The evaluation process typically follows a systematic approach.
Initial Assessment and Blood Pressure Confirmation
The first step involves confirming that blood pressure is genuinely elevated and not due to measurement error or white coat hypertension. Home blood pressure monitoring and ambulatory blood pressure monitoring can help distinguish true resistant hypertension from pseudoresistance.
Medication Review
A thorough review of all current medications is essential, including blood pressure medications and other prescription and over-the-counter drugs that may interfere with blood pressure control. This review often identifies medications contributing to treatment resistance that can be discontinued or substituted.
Secondary Cause Investigation
When pseudoresistance has been excluded and medications have been optimized, investigation for secondary causes of hypertension becomes necessary. Diagnostic testing may include blood and urine studies to assess kidney function, hormone levels, and electrolytes. Imaging studies such as renal artery ultrasound or CT angiography may be performed to evaluate for renal artery stenosis.
Comprehensive Treatment Approach
Successful management of resistant hypertension requires identification and reversal of lifestyle factors contributing to treatment resistance, appropriate diagnosis and treatment of secondary causes, and optimization of antihypertensive medication regimens.
Lifestyle Modifications
Lifestyle changes remain the foundation of resistant hypertension management and should be implemented alongside pharmacological therapy. Key lifestyle modifications include:
– Reducing dietary sodium intake to less than 2,300 mg daily- Maintaining a healthy weight through caloric restriction and weight loss- Engaging in regular aerobic physical activity- Limiting alcohol consumption- Smoking cessation- Managing stress through relaxation techniques- Treating obstructive sleep apnea if present- Keeping a home blood pressure log for monitoring- Attending educational workshops about hypertension management
These modifications should be reinforced consistently and supported by comprehensive support services including dietary counseling, exercise recommendations, and stress reduction programs.
Medication Optimization
When lifestyle modifications alone are insufficient, medication adjustments become necessary. The first step often involves increasing the diuretic dose, as volume overload is a common but underappreciated cause of treatment resistance. For patients with adequate kidney function, thiazide or thiazide-like diuretics are preferred.
If blood pressure remains uncontrolled with three medications, a fourth medication should be added. An aldosterone antagonist such as spironolactone is frequently recommended as the fourth agent, particularly in patients with appropriate potassium levels. The most commonly used antihypertensive medication classes include:
– Diuretics (thiazide, loop, and potassium-sparing)- Angiotensin-converting enzyme (ACE) inhibitors- Angiotensin II receptor blockers (ARBs)- Beta-blockers- Calcium channel blockers- Aldosterone antagonists
Some patients with resistant hypertension may require four or five different blood pressure medications to achieve adequate control.
Advanced and Emerging Treatments
For patients who remain uncontrolled despite optimized medical therapy, several advanced treatment options are now available or in development.
Renal Denervation
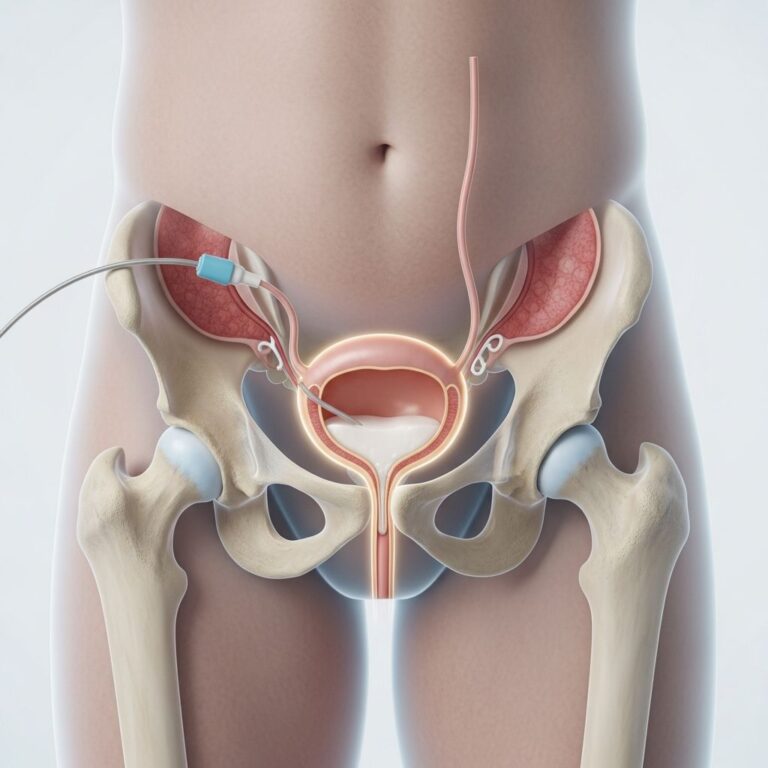
Renal denervation represents a promising minimally invasive treatment for resistant hypertension currently undergoing clinical trials. This procedure targets the nerves near the kidneys that are responsible for regulating blood pressure. Unlike earlier surgical approaches that severed renal artery nerves and resulted in excessive blood pressure lowering, modern renal denervation selectively silences specific targeted nerves to restore healthy blood pressure regulation.
The procedure uses heat energy delivered through a catheter—a thin tube threaded through an artery—to ablate specific nerve fibers. Renal denervation is minimally invasive compared to traditional surgical approaches and offers potential benefits for carefully selected patients who have failed standard medical therapy.
Specialized Management Programs
Resistant hypertension should be managed at specialized centers with expertise in complex hypertension cases. These programs typically provide dedicated follow-up care, active clinical research participation to evaluate new treatments, and comprehensive support services to help patients cope with their diagnosis and maintain adherence to treatment plans.
Health Consequences and Complications
Untreated or inadequately controlled resistant hypertension significantly increases the risk of serious health complications. These include myocardial infarction (heart attack), cerebrovascular accident (stroke), progressive kidney damage leading to chronic kidney disease or end-stage renal disease, and left ventricular hypertrophy.
The longer blood pressure remains uncontrolled, the greater the cumulative damage to the cardiovascular and renal systems. This underscores the importance of early identification, aggressive intervention, and consistent long-term management of resistant hypertension.
Key Points for Patient Success
Achieving success in managing resistant hypertension requires active participation and commitment from patients. Several critical factors contribute to better outcomes:
– Strict adherence to medication regimens, taking medications exactly as prescribed- Regular home blood pressure monitoring to track progress- Consistent lifestyle modifications maintained over time- Open communication with healthcare providers about symptoms and concerns- Attendance at follow-up appointments and educational programs- Active management of other medical conditions, particularly diabetes and chronic kidney disease
Frequently Asked Questions
Q: What is the difference between resistant hypertension and regular high blood pressure?
A: Regular high blood pressure responds well to lifestyle changes and one to two medications. Resistant hypertension persists despite treatment with at least three different blood pressure medications at adequate doses, typically including a diuretic. It often indicates an underlying medical condition requiring specialized investigation.
Q: How common is resistant hypertension?
A: Resistant hypertension affects a significant portion of the hypertensive population. The actual prevalence decreases when pseudoresistant cases are properly screened and excluded from diagnosis.
Q: Can resistant hypertension be cured?
A: While resistant hypertension cannot always be cured, it can be effectively managed with comprehensive treatment addressing underlying causes, optimized medications, and lifestyle modifications. Some secondary causes, when successfully treated, may result in improved blood pressure control.
Q: Why is medication adherence so important in resistant hypertension?
A: Approximately 40% of resistant hypertension cases result from poor medication adherence. Blood pressure medications must be taken daily at the correct dose and frequency to be effective. Inconsistent medication use can appear as treatment resistance when medications are actually not being taken properly.
Q: What should I do if I have been diagnosed with resistant hypertension?
A: Seek evaluation at a specialized hypertension center for comprehensive assessment. Follow all medication instructions carefully, implement lifestyle modifications, keep a home blood pressure log, attend follow-up appointments, and maintain open communication with your healthcare provider about your condition and treatment response.
Q: Is renal denervation an effective treatment for resistant hypertension?
A: Renal denervation is a promising minimally invasive treatment currently in clinical trials at medical centers nationwide. While early results are encouraging, it is typically considered for select patients who have failed optimized medical therapy and pseudoresistance has been excluded.
References
- Symptoms of Resistant Hypertension — Stanford Healthcare. 2024. https://stanfordhealthcare.org/medical-conditions/blood-heart-circulation/resistant-hypertension/symptoms.html
- Resistant Hypertension: Diagnosis, Evaluation, and Treatment — American Heart Association Journal of Hypertension. 2009. https://www.ahajournals.org/doi/10.1161/hypertensionaha.108.189141
- Why Resistant Hypertension Requires Specialized Management — Prime Internal Medicine Associates. 2025-01-03. https://www.primeinternalmedassociates.com/2025/01/03/why-resistant-hypertension-requires-specialized-management/
- Resistant Hypertension Has Several Possible Causes — Mayo Clinic Newsnetwork. 2024. https://newsnetwork.mayoclinic.org/discussion/resistant-hypertension-has-several-possible-causes/
- Resistant Hypertension: Causes, Symptoms & Treatment — Cleveland Clinic. 2024. https://my.clevelandclinic.org/health/diseases/15601-resistant-hypertension
- High Blood Pressure That’s Hard to Treat — American Heart Association. 2024. https://www.heart.org/en/health-topics/high-blood-pressure/the-facts-about-high-blood-pressure/resistant-hypertension–high-blood-pressure-thats-hard-to-treat
- What is New in Resistant Hypertension — European Society of Cardiology. 2024. https://www.escardio.org/Councils/Council-for-Cardiology-Practice-(CCP)/Cardiopractice/what-is-new-in-resistant-hypertension
Similar Articles






Read full bio of medha deb