Retinoblastoma: A Parent’s Guide To Early Signs And Treatment
Discover the causes, symptoms, diagnosis, and life-saving treatments for retinoblastoma, the rare childhood eye cancer affecting the retina.

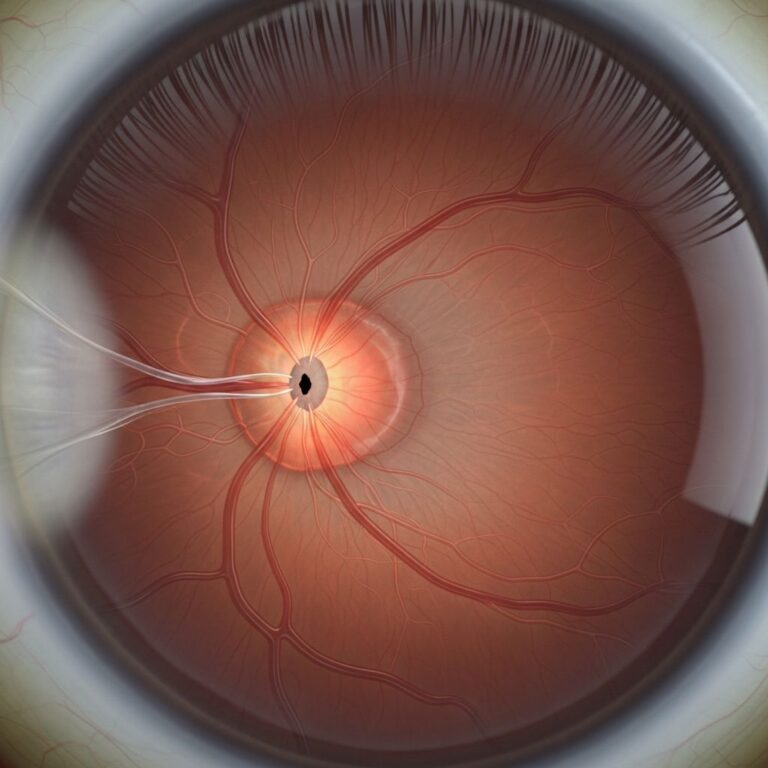
Retinoblastoma represents one of the most common intraocular cancers in infants and young children, originating in the retina—the light-sensitive tissue lining the back of the eye. This aggressive malignancy arises from immature retinal cells that lose normal growth controls, leading to tumor formation that can threaten vision and life if not addressed promptly. With advances in medical science, survival rates now surpass 95% in developed regions when detected early.
The Genetic Roots of Retinoblastoma
At the core of retinoblastoma lies a disruption in the RB1 tumor suppressor gene, located on chromosome 13q14. This gene produces a protein called pRB, which acts as a cellular brake, preventing excessive division by blocking progression from the G1 to S phase in the cell cycle. When both copies of RB1 are inactivated—following Knudson’s two-hit hypothesis—retinal cells proliferate uncontrollably, forming tumors.
Hereditary retinoblastoma, accounting for about 45% of cases, involves a germline mutation in one RB1 allele inherited from a parent or arising de novo. The second hit occurs somatically in retinal cells, often resulting in bilateral (both eyes) or multifocal tumors presenting earlier in life, typically before age 1. Nonhereditary cases (55%) require two somatic mutations within the same retinal cell, leading to unilateral tumors that appear later, around age 2.
Rarely, roughly 2% of tumors develop independently of RB1 through MYCN oncogene amplification, causing rapid, aggressive unilateral growth in very young infants.
Who Is at Risk? Incidence and Demographics
Retinoblastoma strikes approximately 1 in 15,000 to 20,000 live births worldwide, with no strong racial or geographic bias, though incidence varies slightly by region due to detection capabilities. Nearly all cases occur in children under 5, peaking between 6 and 24 months. Boys and girls are equally affected.
- Hereditary risk: Family history elevates odds; affected siblings or parents pass the mutation with 50% autosomal dominant probability, though penetrance nears 90%.
- Sporadic cases: Most common, with no family link; advanced paternal age weakly correlates via sperm DNA errors.
- Trilateral form: Rare extension to pineal gland, linked to hereditary types.
Environmental factors like prenatal radiation or chemicals show limited causation evidence, emphasizing genetics as the primary driver.
Recognizing the Signs: Symptoms and Early Detection
Early symptoms often evade notice since young children rarely complain of vision loss. The hallmark is leukocoria, a white pupil reflex instead of red in flash photos, visible in 60% of cases. Other indicators include:
- Strabismus (crossed or wandering eye) from tumor interference with eye alignment.
- Red, painful eye with inflammation if tumor invades anterior structures.
- Decreased vision, poor pupil response, or nystagmus (eye jiggling).
- Rarely, proptosis (bulging eye) or orbital inflammation in advanced disease.
Parents and pediatricians should routinely check red reflex with a direct ophthalmoscope at well-child visits. Delayed diagnosis heightens risks of metastasis to brain or bone.
How Doctors Diagnose Retinoblastoma
Diagnosis hinges on comprehensive ophthalmic exam under anesthesia, using indirect ophthalmoscopy to visualize retinal masses—often white-yellow with calcification. Key imaging modalities include:
| Modality | Purpose | Advantages |
|---|---|---|
| Ultrasound (B-scan) | Detects calcification, tumor size | Non-invasive, quick |
| MRI | Assesses extraocular spread, trilateral disease | Soft tissue detail, no radiation |
| CT (less common) | Calcification confirmation | Radiation exposure limits pediatric use |
| Fluorescein angiography | Vascular patterns | Identifies feeders for targeted therapy |
Genetic testing confirms RB1 status via blood or tumor biopsy, guiding family screening. Staging employs International Classification (group A-E) for intraocular extent and Reese-Ellsworth for treatment planning.
Treatment Strategies: Saving Eyes and Lives
Multidisciplinary care at specialized centers prioritizes globe salvage, vision preservation, and cure. Options escalate by tumor size, location, and spread:
- Focal therapies (small tumors): Cryotherapy freezes tumors; laser photocoagulation seals vessels; thermotherapy heats precisely.
- Intra-arterial chemotherapy (IAC): Delivers drugs like melphalan directly to ophthalmic artery, revolutionizing unilateral salvage rates to 70-90%.
- Systemic chemotherapy: Vincristine, etoposide, carboplatin shrink larger tumors pre-focal therapy.
- Enucleation: Surgical eye removal for advanced unilateral or blind painful eyes; prosthetic fitting follows.
- EBRT (external beam radiotherapy): Reserved for recurrence due to secondary cancer risks.
Success hinges on early intervention; unilateral cure nears 100%, bilateral 95% overall. Metastatic cases (rare, <5%) require intensive chemo, radiation, and stem cell transplant.
Life After Treatment: Follow-Up and Complications
Survivors face lifelong surveillance for recurrence (first 5 years critical) and secondary cancers—osteosarcoma, melanoma, lung—elevated 10-20x in hereditary cases due to RB1 dysfunction. Annual exams include dilated funduscopy, MRI for trilateral risk.
Other concerns:
- Vision impairment or blindness in treated eye.
- Cosmetic issues post-enucleation, addressed by implants.
- Psychosocial impacts; counseling aids coping.
- Fertility preservation pre-chemo for future families.
Genetic counseling is vital: Hereditary carriers have 50% transmission risk; prenatal/preimplantation testing available.
Prevention and Family Screening Guidelines
While unpreventable genetically, proactive screening transforms outcomes. For family history:
- Exam under anesthesia every 2 months age 0-12 months, then 3-4 months to age 3, biannually to 7.
- Genetic testing identifies at-risk relatives.
Public education on leukocoria via “Red Reflex Test” campaigns boosts early detection.
FAQs About Retinoblastoma
What is the survival rate for retinoblastoma?
Over 95% in high-resource settings with timely care; lower in developing areas due to late presentation.
Can retinoblastoma be cured without removing the eye?
Yes, intra-arterial chemo and focal therapies save 70-90% of eyes in early stages.
Is retinoblastoma hereditary?
About 45% yes (bilateral often); 55% sporadic (unilateral usually).
How do I check my child’s pupils at home?
Take flash photos in dim light; white glow instead of red warrants immediate pediatrician visit.
Does retinoblastoma affect adults?
Extremely rare; almost exclusively pediatric under age 5.
Emerging Frontiers in Retinoblastoma Care
Ongoing research targets RB1-independent pathways like MYCN, exploring targeted inhibitors, gene therapy to restore pRB function, and nanoparticle drug delivery for precision. Global initiatives aim to equalize outcomes via telemedicine screening and affordable chemo.
This comprehensive approach underscores retinoblastoma’s curability, transforming a once-fatal diagnosis into a manageable condition with vigilant care.
References
- Retinoblastoma – StatPearls – NCBI Bookshelf — National Center for Biotechnology Information. 2023-07-17. https://www.ncbi.nlm.nih.gov/books/NBK545276/
- Retinoblastoma: Symptoms & Treatment — Cleveland Clinic. 2023-11-01. https://my.clevelandclinic.org/health/diseases/retinoblastoma
- Causes, Risk Factors, and Prevention of Retinoblastoma — American Cancer Society. 2024-02-12. https://www.cancer.org/cancer/types/retinoblastoma/causes-risks-prevention.html
- Retinoblastoma – Symptoms, Causes, Treatment | NORD — National Organization for Rare Disorders. 2023-05-15. https://rarediseases.org/rare-diseases/retinoblastoma/
- Retinoblastoma (Eye Cancer in Children) — Children’s Hospital of Philadelphia. 2024-01-10. https://www.chop.edu/conditions-diseases/retinoblastoma
- Retinoblastoma | National Eye Institute – NIH — National Eye Institute. 2023-09-20. https://www.nei.nih.gov/eye-health-information/eye-conditions-and-diseases/retinoblastoma
- Retinoblastoma – Symptoms and causes — Mayo Clinic. 2023-12-05. https://www.mayoclinic.org/diseases-conditions/retinoblastoma/symptoms-causes/syc-20351008
Similar Articles






Read full bio of medha deb