Scleritis: Inflammation of the Eye’s Protective Layer
A comprehensive guide to understanding scleritis symptoms, types, and treatment options

Defining the Condition
The sclera, commonly known as the white of the eye, serves as a protective fibrous layer that maintains the eye’s structural integrity and shields delicate internal components. When this crucial tissue becomes inflamed, a condition called scleritis develops. This is not a minor irritation; scleritis represents a serious inflammatory disorder that demands prompt medical attention and specialized care. Unlike superficial eye conditions that resolve independently, scleritis can lead to permanent vision damage if left untreated.
Scleritis is classified as a rare condition, though its prevalence appears to be increasing in clinical practice. The inflammation characteristic of scleritis penetrates deep into the scleral tissue, distinguishing it from milder ocular surface conditions. Approximately one-third of patients diagnosed with scleritis have an underlying systemic inflammatory or autoimmune condition, indicating that this eye disease frequently signals broader health concerns requiring comprehensive medical evaluation.
The Two Primary Categories of Scleritis
Medical professionals divide scleritis into two main categories based on the anatomical location of inflammation. Understanding these distinctions is essential for diagnosis and determining appropriate treatment strategies.
Anterior Scleritis: The More Common Form
Anterior scleritis accounts for approximately 90% of all scleritis cases and involves inflammation of the scleral tissue located in front of the eye’s extraocular muscles. The inflammatory changes in this region are typically visible during clinical examination, allowing eye care professionals to observe redness and swelling directly. This visibility often facilitates earlier diagnosis compared to posterior forms of the disease.
Within the anterior scleritis category, three distinct subtypes exist, each presenting unique clinical features and treatment considerations:
- Diffuse anterior scleritis represents the most prevalent subtype and spreads across the anterior scleral surface with widespread inflammation and swelling. This form generally demonstrates better treatment responsiveness and offers a more favorable prognosis than more severe variants.
- Nodular anterior scleritis produces localized inflamed bumps or nodules on the eye’s white surface. These tender nodules cause discomfort when directly touched and appear as distinct lesions during examination.
- Necrotizing anterior scleritis is the most destructive form, characterized by actual tissue death and melting of scleral material. In severe cases, this can expose deeper ocular structures and create visible holes in the sclera itself, representing the worst prognosis among anterior scleritis variants.
Posterior Scleritis: The Hidden Inflammation
Posterior scleritis affects the scleral tissue behind the eye’s extraocular muscles, making it significantly more difficult to detect through standard clinical examination. Because inflammation occurs in a deeper, less visible location, posterior scleritis is often diagnosed later in disease progression. Despite its rarity compared to anterior forms, posterior scleritis can cause serious complications including retinal detachment, angle-closure glaucoma, and substantial vision loss when not promptly addressed.
Clinical Presentation and Symptoms
Patients with scleritis typically experience a distinctive clinical presentation that should trigger immediate medical evaluation. The symptoms of scleritis are notably more severe than common eye conditions, and this intensity serves as an important diagnostic clue for both patients and healthcare providers.
Pain characteristics represent the hallmark symptom of scleritis. The pain is typically described as a deep, boring sensation that intensifies with eye movement and often worsens during nighttime hours, potentially disrupting sleep. In some cases, particularly with necrotizing variants, pain may be surprisingly minimal despite significant tissue damage occurring. The pain frequently radiates beyond the eye itself, affecting the eyebrow region, temple, jaw, or adjacent facial areas.
Visual changes accompany the pain in many cases. Patients report blurred vision as inflammation affects optical clarity, and in more advanced cases, progressive vision loss may occur. The severity of visual symptoms correlates with the extent and location of scleral involvement and any secondary inflammation affecting adjacent ocular structures.
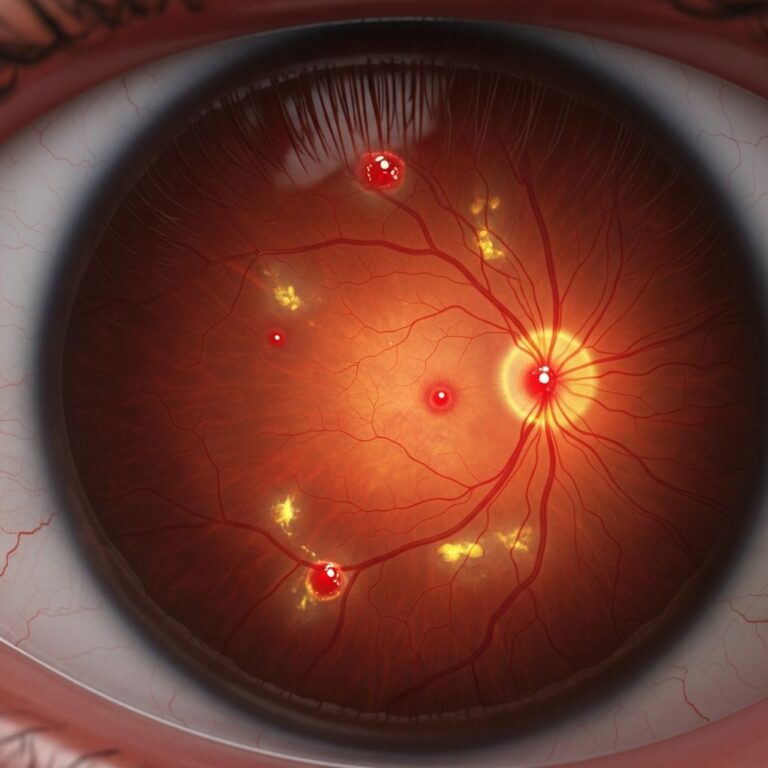
Redness and appearance differ notably from typical conjunctivitis or pink eye. Rather than the bright pink or red appearance of surface inflammation, scleritis typically produces a deeper, purple-tinged or bluish-red discoloration. In some instances, areas of the sclera may appear thin, dark, or even translucent due to tissue loss.
Photophobia, an exaggerated sensitivity to light, commonly accompanies scleritis. This light sensitivity can be severe enough that patients find normal indoor lighting uncomfortable and may prefer dimmed environments.
Additional symptoms may include excessive tearing unrelated to emotional responses or allergies, tenderness around the eye that makes wearing glasses uncomfortable, and a persistent sensation of a foreign object in the eye. Some patients experience double vision, though this is less common than other symptoms.
Underlying Causes and Risk Factors
Scleritis frequently develops as a manifestation of systemic disease rather than as an isolated eye condition. Understanding the underlying causes helps explain why comprehensive medical evaluation is essential for all patients diagnosed with scleritis.
Autoimmune and inflammatory diseases represent the most common underlying associations with scleritis. Rheumatoid arthritis occurs in a significant proportion of scleritis patients, with the eye inflammation sometimes appearing as the initial manifestation of the systemic disease. Other autoimmune conditions frequently linked to scleritis include inflammatory bowel disease, systemic lupus erythematosus, granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis), and scleroderma.
Infectious triggers can precipitate scleritis development in some patients. Long-standing infections elsewhere in the body may activate immune responses that affect ocular tissues. Additionally, ocular trauma or injury can initiate scleritis in susceptible individuals. Some cases appear idiopathic, with no identifiable triggering factor despite thorough investigation.
Demographic factors influence scleritis presentation. The condition predominantly affects middle-aged individuals, with women experiencing scleritis more frequently than men. Scleritis may initially affect one eye but can subsequently develop in the contralateral eye during the same disease episode or in later recurrent episodes.
Diagnostic Approach and Evaluation
Accurate diagnosis of scleritis requires specialized examination techniques and clinical expertise. Eye care professionals employ several diagnostic modalities to confirm scleritis and classify its type.
Slit lamp biomicroscopy represents the primary diagnostic tool, allowing detailed visualization of the sclera and anterior ocular structures under magnification. During slit lamp examination, clinicians observe characteristic features including scleral vessel patterns that do not blanch with topical phenylephrine (a distinguishing feature from episcleritis), the specific location and pattern of inflammation, and evidence of tissue changes or necrosis.
Comprehensive eye examination including dilated fundus evaluation helps identify any secondary inflammation affecting the cornea, iris, ciliary body, or posterior segment. Such secondary involvement carries prognostic implications and influences treatment decisions.
Imaging studies such as ultrasound B-scan or magnetic resonance imaging may be employed to evaluate posterior scleritis, which is challenging to visualize with conventional methods. These imaging techniques help detect posterior scleral thickening, inflammation, and associated complications.
Systemic evaluation is crucial given the frequent association between scleritis and systemic disease. Appropriate laboratory testing, imaging, and rheumatologic consultation help identify underlying autoimmune or infectious conditions requiring treatment. This comprehensive approach often reveals previously undiagnosed systemic disease.
Treatment Strategies and Management Approaches
Treatment of scleritis requires a multimodal approach tailored to disease severity, type, and any identified underlying systemic conditions. Self-limited resolution does not occur in scleritis; active intervention is necessary to prevent permanent vision loss.
Corticosteroid therapy forms the foundation of scleritis treatment. Systemic corticosteroids, typically administered orally, provide the anti-inflammatory effect necessary to control inflammation and prevent tissue destruction. The specific steroid dose and duration depend on disease severity and response to therapy. Topical corticosteroid drops provide supplementary benefit but cannot serve as monotherapy for scleritis.
Nonsteroidal anti-inflammatory medications may be incorporated into treatment regimens, particularly for pain management and as adjunctive therapy to corticosteroids. These agents help reduce inflammation and improve comfort, though they are typically insufficient as sole treatment.
Immunosuppressive agents are frequently necessary, particularly for severe cases, necrotizing scleritis, or when corticosteroids alone prove insufficient. Medications such as methotrexate, azathioprine, and biologic agents help control the underlying inflammatory process and may reduce steroid requirements.
Management of underlying disease is essential when systemic conditions precipitate scleritis. Appropriate treatment of rheumatoid arthritis, inflammatory bowel disease, or other autoimmune conditions improves ocular outcomes and reduces scleritis recurrence rates.
Topical antibiotics may be prescribed when secondary bacterial infection is suspected, though scleritis itself is not typically bacterial in etiology.
Comparison with Similar Eye Conditions
Scleritis is frequently confused with other red eye conditions, yet distinction is clinically important as treatment approaches differ substantially.
| Feature | Scleritis | Episcleritis | Conjunctivitis (Pink Eye) |
|---|---|---|---|
| Pain Severity | Severe, deep pain | Mild to moderate discomfort | Minimal pain |
| Redness Appearance | Deep purple or blue-red | Bright red or pink | Bright red or pink |
| Vision Impact | Often affected | Not affected | Usually not affected |
| Vessel Blanching | Vessels do not blanch | Vessels blanch with drops | Vessels blanch easily |
| Depth of Involvement | Deep scleral inflammation | Episcleral layer only | Surface conjunctiva only |
| Treatment Urgency | Emergency; immediate care needed | Non-urgent | Symptomatic care; often self-limited |
Potential Complications and Long-Term Outcomes
Without appropriate treatment, scleritis can lead to serious ocular complications. Understanding these potential outcomes underscores the importance of early diagnosis and aggressive management.
Vision loss represents the most significant long-term consequence. This can occur through direct inflammation affecting the cornea or optic nerve, or secondary complications such as glaucoma development or retinal detachment. In necrotizing scleritis, permanent blindness in the affected eye is possible.
Scleral perforation can occur in severe necrotizing cases, creating an actual hole in the sclera. This represents an ocular emergency requiring specialized surgical management to prevent catastrophic vision loss.
Secondary inflammation may develop, with the inflammation extending to involve the cornea (sclerazing keratitis), uvea, or other adjacent structures, compounding vision risk.
Glaucoma may develop as a secondary consequence of scleritis or associated inflammation, requiring ongoing monitoring and potential additional treatment.
Frequently Asked Questions
Can scleritis resolve without treatment?
No. Scleritis is a serious condition requiring active medical intervention. Attempting to manage scleritis without professional treatment risks permanent vision loss and disease progression.
Is scleritis contagious?
Scleritis is not contagious. It is an inflammatory condition without infectious etiology in most cases, therefore cannot be transmitted to other individuals.
How long does scleritis treatment typically last?
Treatment duration varies considerably depending on disease severity and type. Some cases resolve within weeks to months, while others require prolonged therapy lasting many months or years, particularly when immunosuppressive agents are necessary.
Will scleritis return after treatment?
Recurrence is possible, particularly if underlying systemic disease remains uncontrolled. Some patients experience isolated episodes, while others have repeated recurrences requiring long-term management strategies.
Can both eyes be affected simultaneously?
Yes. Scleritis may initially present unilaterally but can develop bilaterally during the same disease episode. Some patients experience sequential involvement, with one eye affected initially and the other affected in later recurrences.
What role does systemic disease evaluation play in scleritis management?
Systemic disease evaluation is essential since approximately one-third of scleritis patients have underlying autoimmune or inflammatory disease. Identifying and treating these conditions improves ocular outcomes and reduces recurrence rates.
References
- Scleritis – Clinical Management Guideline — College of Optometrists. 2024. https://www.college-optometrists.org/clinical-guidance/clinical-management-guidelines/scleritis
- Scleritis — StatPearls, National Center for Biotechnology Information, U.S. National Library of Medicine. 2025. https://www.ncbi.nlm.nih.gov/books/NBK499944/
- Scleritis: What It Is, Causes, Symptoms & Treatment — Cleveland Clinic. 2024. https://my.clevelandclinic.org/health/diseases/24975-scleritis
- Scleritis and Episcleritis — Taming the SRU. 2024. https://www.tamingthesru.com/blog/bread-butter-em/scleritis-and-episcleritis
- Scleritis: A Quick Guide — Review of Optometry. 2019. https://www.reviewofoptometry.com/CMSDocuments/2019/06/ScleritisGuide.pdf
- Scleritis: Care Instructions — MyHealth Alberta. 2024. https://myhealth.alberta.ca/Health/aftercareinformation/pages/conditions.aspx?hwid=abq6325
Similar Articles






Read full bio of Sneha Tete