Squamous Cell Papilloma: Causes, Diagnosis & Treatment Guide
Comprehensive guide to squamous cell papilloma: causes, symptoms, diagnosis, and effective treatment options for this common benign skin growth.

What is squamous cell papilloma?
Squamous cell papilloma is a benign epithelial tumour caused by human papillomavirus (HPV) infection. It typically presents as a firm, skin-coloured, wart-like papule with a rough surface, often found on the hands, face, or neck. These lesions are generally asymptomatic and have a low risk of malignant transformation, particularly when associated with low-risk HPV types such as 6 and 11.
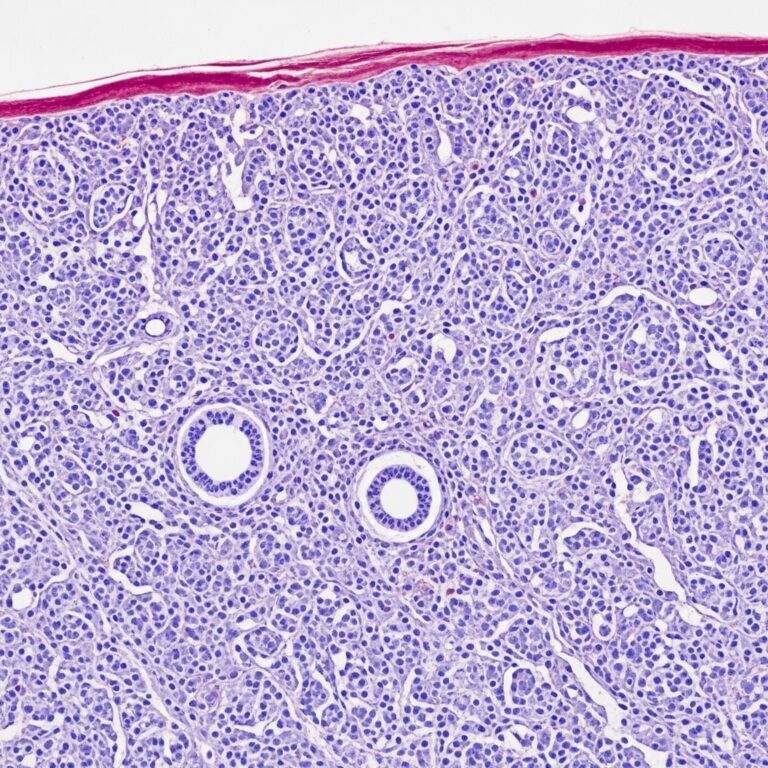
Histologically, squamous cell papillomas exhibit acanthosis, papillomatosis, and hyperkeratosis, characteristic features of HPV-induced epithelial proliferation. While most common on cutaneous sites, similar lesions can occur in the oral cavity, where they may present as painless, pedunculated growths.
Who gets squamous cell papilloma?
Squamous cell papilloma affects individuals of all ages but is more prevalent in adults due to cumulative exposure to HPV. Risk factors include:
- Direct contact with HPV-infected skin or mucous membranes.
- Immunosuppression, such as in HIV/AIDS or transplant patients, increasing susceptibility to persistent HPV infection.
- Occupations involving frequent hand contact, like healthcare workers or gardeners.
- Poor hygiene or shared personal items in communal settings.
Children and young adults may develop lesions following minor trauma or autoinoculation from common warts. Oral squamous papillomas are frequently linked to oral sex or close contact with infected individuals.
What causes squamous cell papilloma?
The primary aetiology is infection with
low-risk HPV types
, particularly HPV-6 and HPV-11, which induce hyperplasia without oncogenic potential. These subtypes account for over 90% of oral squamous cell papillomas.HPV enters the basal layer of the epithelium through microtrauma, leading to viral DNA replication in keratinocytes. This triggers abnormal cell proliferation, resulting in the characteristic papillary architecture. Unlike high-risk HPV types (16, 18), low-risk strains rarely progress to dysplasia or squamous cell carcinoma.
Transmission occurs via skin-to-skin contact, fomites, or autoinoculation. In oral sites, sexual transmission is a key route.
What are the clinical features of squamous cell papilloma?
Cutaneous lesions appear as:
- Firm, dome-shaped or filiform papules (2–5 mm).
- Rough, verrucous surface resembling a common wart.
- Skin-coloured to white; occasionally hyperpigmented.
- Locations: dorsum of hands, fingers, face, eyelids, neck.
Oral squamous papillomas present as:
- Soft, pedunculated or sessile growths on tongue, palate, buccal mucosa, gingiva, or lips.
- White, cauliflower-like surface; typically 5–10 mm.
- Usually solitary but can be multiple.
Lesions are painless, non-ulcerated, and do not impair function unless large. Rare complications include secondary infection or cosmetic concerns.
| Location | Appearance | Size | Symptoms |
|---|---|---|---|
| Cutaneous (hands, face) | Firm papule, verrucous | 2–5 mm | Asymptomatic |
| Oral cavity | Pedunculated, cauliflower | 5–20 mm | Mild irritation if large |
| Anogenital | Condyloma-like | Variable | Itching, bleeding |
How is squamous cell papilloma diagnosed?
Diagnosis is primarily clinical, based on characteristic morphology and history of HPV exposure. Dermoscopy may reveal a mosaic pattern or comma-like vessels.
Biopsy is reserved for:
- Atypical features or diagnostic uncertainty.
- High-risk sites (anogenital, oropharynx).
- Recurrent or rapidly growing lesions.
Histopathology confirms koilocytes (HPV-infected cells with perinuclear halos), papillomatosis, and orderly maturation without atypia. HPV typing via PCR identifies subtypes.
Differential diagnosis includes seborrhoeic keratosis, verruca vulgaris, molluscum contagiosum, and rarely, squamous cell carcinoma.
What is the treatment for squamous cell papilloma?
Many lesions regress spontaneously within 1–2 years, especially in immunocompetent patients. Treatment is indicated for symptomatic, cosmetic, or diagnostic concerns.
Conservative surgical excision
The gold standard: complete removal of the lesion head and base using scalpel or scissors under local anaesthesia. Recurrence is unlikely (<5%) with clear margins.
Other treatment options
- Cryotherapy: Liquid nitrogen freezing (-196°C) causes tissue necrosis. 1–2 cycles; effective for small lesions with minimal scarring.
- Laser ablation: CO2 or pulsed-dye laser vaporizes tissue precisely. Ideal for facial or oral lesions; excellent cosmesis.
- Electrosurgery/curettage: Electrodesiccation followed by curettage for cutaneous sites.
- Topical therapies: Imiquimod (immune modulator) or podophyllin for multiple lesions; less effective for solitary papillomas.
For oral papillomas, endoscopic excision or laser is preferred to preserve function.
Complications of squamous cell papilloma
Benign course with rare complications:
- Recurrence (5–10%) if incomplete removal.
- Secondary bacterial infection.
- Cosmetic scarring post-treatment.
- Extremely low risk of malignant transformation (<1%) with HPV-6/11.
High-risk HPV subtypes or immunosuppression elevate progression risk to dysplasia.
Prevention of squamous cell papilloma
Key strategies:
- HPV vaccination: Quadrivalent (Gardasil) or nonavalent vaccines target HPV-6/11, preventing 90% of lesions. Recommended ages 9–45.
- Avoid skin-to-skin contact with warts.
- Hand hygiene and not sharing razors/towels.
- Smoking cessation, as it impairs HPV clearance.
Further reading and references
For in-depth histopathology, see pathology outlines on verrucous lesions. Patient resources on HPV vaccination from CDC/WHO.
Frequently Asked Questions
Q: Is squamous cell papilloma cancerous?
No, it is a benign growth caused by low-risk HPV types with negligible malignant potential.
Q: Do squamous cell papillomas go away on their own?
Yes, many resolve spontaneously within 1–2 years via immune clearance.
Q: What is the best treatment for oral papilloma?
Surgical excision or laser ablation; recurrence is rare with complete removal.
Q: Can HPV vaccines prevent skin papillomas?
Yes, vaccines covering HPV-6/11 significantly reduce risk.
Q: How do you get rid of a papilloma on the hand?
Cryotherapy, excision, or salicylic acid; consult a dermatologist.
References
- Squamous Papilloma: Causes, Symptoms, and Treatments — Docus.ai (Dr Anna Nersisyan, reviewed Dr George Laliotis). 2025-04-18. https://docus.ai/symptoms-guide/squamous-papilloma
- Papillomas: A Multisystem Overview — StatPearls (NCBI Bookshelf). 2023-07-17. https://www.ncbi.nlm.nih.gov/books/NBK560737/
- Squamous cell papilloma — DermNet NZ. 2024 (accessed). https://dermnetnz.org/topics/squamous-cell-papilloma
- Oral Papilloma Treatment for HPV Infection — PO Dental. 2024. https://www.pomdental.com/oral-papilloma-treatment/
- Management of an Oral Squamous Cell Papilloma in an Unusual Maxillofacial Location: A Case Report — Cureus. 2024. https://www.cureus.com/articles/447225-management-of-an-oral-squamous-cell-papilloma-in-an-unusual-maxillofacial-location-a-case-report
Similar Articles






Read full bio of medha deb