Surgical Repair of Nerves: Procedures and Recovery
Learn about nerve surgery options, procedures, timing, and recovery for peripheral nerve injuries.

Surgical Repair of Nerves: Comprehensive Guide to Treatment and Recovery
Peripheral nerve injuries can result from trauma, accidents, compression, or medical conditions that damage the delicate nerve fibers responsible for transmitting signals between your brain, spinal cord, and the rest of your body. When these injuries prevent normal function, surgical repair may be necessary to restore sensation, movement, and quality of life. Understanding the various surgical approaches, timing considerations, and recovery expectations can help patients make informed decisions about their treatment options.
Understanding Peripheral Nerve Injuries
Peripheral nerves are responsible for carrying signals that control movement and sensation throughout the body. When these nerves are damaged through crushing, stretching, cutting, or compression, they may lose their ability to transmit signals effectively. The severity of a nerve injury determines whether conservative treatment or surgical intervention is necessary.
Nerve injuries initiate a series of regenerative and degenerative processes within the body. When these processes fail to proceed in a synchronized manner, complications such as neuroma formation or persistent nerve deficiency may occur, both of which can be progressive in nature. Early assessment and appropriate intervention become critical to preventing long-term complications.
When is Surgical Repair Recommended?
Not all nerve injuries require surgery. Your healthcare provider will evaluate your condition based on several factors to determine if operative intervention is necessary. Surgical repair is typically recommended when:
– The nerve is completely severed or transected- Nerve compression symptoms are rapidly progressing- There is significant loss of function in the affected area- Conservative treatment has failed to produce improvement- Diagnostic testing shows the nerve cannot regenerate on its own- Functional deficits, pain, or muscle atrophy are worsening despite non-surgical management
Your surgeon will perform diagnostic tests, including electromyography (EMG) and nerve conduction studies, to assess nerve function and determine the extent of damage. These tests help guide the decision regarding surgical timing and approach.
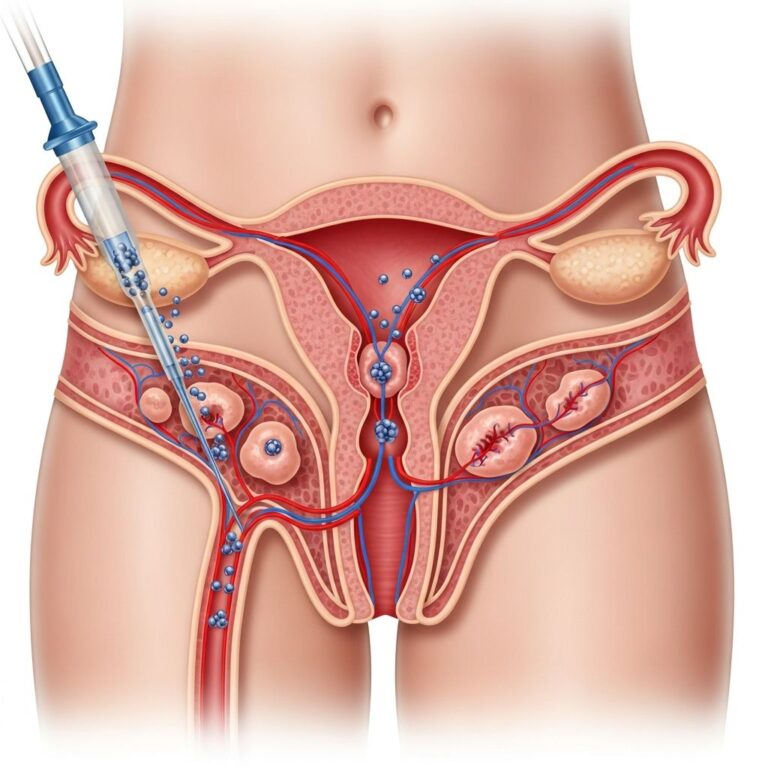
Diagnostic Assessment During Surgery
During surgical evaluation, surgeons utilize intraoperative nerve action potential (NAP) recording to assess nerve viability. This diagnostic tool involves inserting electrodes into the body to determine whether injured nerves respond to electrical stimulation. If the nerve responds to the electrical pulse, this indicates that the nerve remains functional and may regenerate independently. The absence of a signal tells the surgeon that the nerve cannot regenerate on its own and requires reconstruction.
Recent innovations in nerve assessment have improved surgical decision-making. Biomedical engineers at Johns Hopkins have developed electrode sets designed to work without requiring surgeons to move or lift the nerve during evaluation, reducing the risk of patient injury and improving the accuracy of readings. This advancement helps streamline neurosurgical workflows and allows surgeons to make better-informed treatment decisions that ultimately decrease patient recovery time and maximize peripheral nerve regeneration.
Timing of Surgical Intervention
The timing of nerve surgery is a critical factor in achieving successful outcomes. Research has established evidence-based guidelines for optimal surgical timing based on the type of nerve injury and symptoms presented.
For nerve decompression procedures treating compression syndromes, surgery should ideally be performed within three to six months from the onset of symptoms. However, if functional deficits, pain, or muscle atrophy are rapidly progressing, acute intervention should be considered even within this window. Additional preoperative factors that influence surgical timing include age, extent of muscle atrophy, grip strength measurements, electrophysiological severity, tobacco use, body mass index, anemia, depression, chronic lung disease, and presence of inflammatory arthritis.
Revision decompression procedures may be planned with careful consideration of symptom severity and the speed of symptom progression. The goal is to intervene before irreversible nerve damage occurs, as untreated nerve injuries can result in lasting changes to sensory, motor, and cognitive function in the brain.
Surgical Repair Methods
Several established surgical techniques are available for repairing peripheral nerves, each with specific indications and outcomes. The choice of repair method depends on the type of injury, length of the nerve gap, location of the injury, and availability of tissue.
Direct Suture Repair
Direct suture repair, also called primary repair, is performed when the nerve ends can be brought together without tension. The surgeon carefully aligns the nerve fibers and uses microsurgical techniques to suture the severed ends together. This method is typically used for clean, recent nerve injuries with minimal nerve loss.
Autograft Reconstruction
When a gap exists between nerve ends that cannot be closed directly, autograft reconstruction involves transplanting a portion of nerve tissue from another part of the patient’s body to bridge the gap. Commonly used donor nerves include the sural nerve from the leg. The advantage of autograft is that the transplanted tissue is the patient’s own tissue, reducing the risk of rejection.
Allograft Reconstruction
Processed nerve allografts, derived from donor tissue that has been treated to remove cells that might trigger immune rejection, provide an effective alternative to autografts for reconstructing peripheral nerve gaps. Research demonstrates that processed nerve allografts offer safe and effective reconstruction for nerve gaps ranging from 5 to 50 millimeters in length.
Studies analyzing outcomes from processed nerve allograft procedures show that overall recovery at functional levels of S3 or M4 and above was achieved in 86% of procedures. Subgroup analysis revealed meaningful levels of recovery in sensory, mixed, and motor nerve repairs, with 89% of digital nerve repairs achieving functional recovery, 75% of median nerve repairs, and 67% of ulnar nerve repairs. These outcomes compare favorably with those reported for nerve autograft and exceed those reported for tube conduits. Notably, there were no reported implant complications, tissue rejections, or adverse experiences related to the use of processed nerve allografts.
Nerve Conduits
Nerve conduits are tubular structures that guide nerve regeneration across gaps. These may be made from biological materials or synthetic compounds and are particularly useful for small nerve gaps. The conduit provides a protected pathway for regenerating nerve fibers to grow toward their target.
Nerve Transfer
In some cases, nerve transfer procedures may be employed, where a healthy nerve branch is redirected to provide input to a damaged nerve. This technique can be beneficial in certain proximal nerve injuries or when multiple nerves are damaged.
Surgical Considerations and Factors
Beyond selecting the appropriate repair method, surgeons must consider several additional factors when planning nerve surgery. These include managing nerve gaps appropriately, considering the ability to reduce resource utilization by performing a single surgery versus staged reconstruction, and managing concomitant injuries or procedures that may be present.
Practical considerations also influence surgical planning, including availability of personal protective equipment, sterile surgical supplies, anesthesia supplies, and staffing. The surgical approach should minimize exposure risks for both the clinical team and patient, extending considerations beyond the surgery itself to recovery room time, hospitalization duration, rehabilitation needs, and efforts to reduce staging of procedures and overall episodes of care.
Socioeconomic factors, insurance coverage, and the likelihood of patients returning for secondary procedures should also be considered when determining the optimal surgical approach, as some treatment plans may require staged procedures over several months.
Managing Nerve Pain and Neuroma
Chronic pain following nerve injury can result from neuroma formation, where scar tissue at the nerve repair site causes pain signals. Successful nerve procedures can improve or eliminate neuropathic pain symptoms while restoring connectivity in the brain’s sensorimotor and salience networks. Timely surgical intervention may reduce the risk of patients progressing to dependence on narcotics or neuromodulators for pain management.
Recovery and Rehabilitation
Recovery following nerve surgery is typically a gradual process that may take several months to years, depending on the extent of the injury and the surgical repair performed. Immediately after surgery, the focus is on protecting the repair site while allowing initial healing. Physical therapy and occupational therapy typically begin within weeks of surgery, focusing on maintaining joint mobility, preventing muscle contraction, and gradually retraining the affected muscles and sensory pathways.
As nerve regeneration progresses, rehabilitation emphasizes functional retraining, sensory re-education, and strengthening exercises. Patients are encouraged to engage in activities that promote normal use of the affected area. Recovery milestones typically occur at 3-6 month intervals, with significant functional improvements often noted within the first year after surgery, though complete recovery may require longer periods.
Factors Affecting Surgical Outcomes
Multiple factors influence the success of nerve surgery. Age, with younger patients generally demonstrating better recovery potential, plays a significant role. The duration between injury and surgery also matters critically—earlier intervention typically produces better results than delayed treatment. The type and location of the nerve injury, extent of muscle atrophy at the time of surgery, and the specific nerve involved all affect expected outcomes.
Patient factors including overall health status, presence of chronic conditions, smoking history, and commitment to rehabilitation also influence recovery. Pre-existing conditions such as diabetes can affect nerve regeneration capacity and should be optimized before surgery when possible.
Frequently Asked Questions
Q: How long does it take to recover from nerve surgery?
A: Recovery timelines vary depending on the type and extent of nerve injury and the surgical repair performed. Initial healing occurs over 2-4 weeks, but meaningful functional recovery typically develops over 3-12 months. Complete recovery may take years as nerve fibers regenerate and reconnect with their targets.
Q: Will I regain full sensation and function after nerve repair?
A: Outcomes depend on multiple factors including the severity of injury, timing of surgery, nerve type, and extent of damage. Many patients achieve significant functional improvement, though complete restoration may not always be possible. Your surgeon can provide individualized expectations based on your specific injury.
Q: What are the risks associated with nerve surgery?
A: Potential risks include infection, bleeding, anesthesia complications, incomplete recovery, and in rare cases, worsening of symptoms. Your surgeon will discuss specific risks related to your procedure and medical history.
Q: Can nerve injuries heal without surgery?
A: Some minor nerve injuries may improve with conservative treatment including rest, physical therapy, and medications. However, complete nerve transections and severe compression injuries typically require surgical repair to restore function.
Q: How is progress monitored after nerve surgery?
A: Progress is monitored through clinical examination, patient-reported functional improvements, and periodic electrophysiological testing (EMG/NCS). Your surgeon will schedule follow-up appointments to assess recovery and adjust rehabilitation as needed.
Q: What is the difference between autograft and allograft nerve repair?
A: Autografts use the patient’s own nerve tissue, reducing rejection risk but requiring harvesting from another body site. Allografts use processed donor tissue, eliminating the need for harvest surgery but require immunosuppression in some cases. Both methods are effective for bridging nerve gaps.
References
- Evidence-Based Approach to Timing of Nerve Surgery: A Review — National Center for Biotechnology Information (NCBI), PubMed Central. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC8560160/
- Functional outcome following nerve repair in the upper extremity — Journal of Hand Surgery. 2012. https://pure.johnshopkins.edu/en/publications/functional-outcome-following-nerve-repair-in-the-upper-extremity–2
- BME Design Team’s innovation aims to improve patient outcomes after peripheral nerve damage — Johns Hopkins University Department of Biomedical Engineering. September 16, 2024. https://www.bme.jhu.edu/news-events/news/design-team-innovation-peripheral-nerve-damage/
- Solutions to the technical challenges embedded in the current methods for intraoperative nerve action potential recording — Johns Hopkins University. https://pure.johnshopkins.edu/en/publications/solutions-to-the-technical-challenges-embedded-in-the-current-met/
Similar Articles






Read full bio of medha deb