Tinea Incognito: 3 Key Steps For Diagnosis And Treatment
Tinea incognito is a masked fungal skin infection altered by steroid use, often misdiagnosed as eczema or rosacea.

What is tinea incognito?
Tinea incognito, also known as tinea incognita, is a superficial fungal infection caused by dermatophytes that presents with an atypical appearance due to modification by topical or systemic corticosteroids, calcineurin inhibitors, or other immunosuppressive agents. The term ‘incognito’ reflects its masked or disguised clinical features, making it challenging to recognize as a fungal infection. Normally, dermatophyte infections like tinea corporis exhibit well-defined annular plaques with central clearing, raised erythematous borders, and scaling; however, steroids suppress the inflammatory response, altering this classic picture.
This condition arises when patients self-treat presumed inflammatory dermatoses such as eczema or psoriasis with potent over-the-counter or prescribed steroids, inadvertently allowing the fungus to spread without typical signs. Systemic steroids or immunosuppressants in patients with underlying conditions can similarly provoke widespread dissemination. Tinea incognito most commonly affects areas where topical steroids are frequently applied, including the face, trunk, extremities, and flexures. Without prompt recognition, it can lead to chronicity, resistance, and secondary complications.
Who gets tinea incognito?
Tinea incognito can affect individuals of any age, gender, or ethnicity, but risk factors include misuse of topical corticosteroids, particularly potent ones applied without medical supervision. It is prevalent in regions with high self-medication rates, such as South Asia and developing countries where over-the-counter steroids are accessible. Patients often have a history of treating presumed eczema, seborrhoeic dermatitis, or contact dermatitis. Immunocompromised individuals, including those on systemic steroids for autoimmune diseases, HIV, or transplant recipients, are at higher risk for disseminated forms.
Children and adults using facial cosmetics with steroids, or those with occupational exposure to fungi (e.g., gardeners, farmers), may also develop it. Genetic predispositions like CARD9 mutations increase susceptibility to severe dermatophytosis. Awareness is crucial in primary care, as misdiagnosis delays antifungal therapy.
What causes tinea incognito?
- Anthropophilic dermatophytes such as Trichophyton rubrum, T. mentagrophytes, T. tonsurans, and Epiderophyton floccosum.
- Less commonly, zoophilic species like Microsporum canis or geophilic fungi.
- In tropical climates, T. violaceum or T. soudanense may predominate.
Steroids inhibit cell-mediated immunity, the primary defense against dermatophytes, allowing fungal proliferation without inflammation. This results in minimal scaling and blurred borders, mimicking non-infectious conditions.
What are the clinical features of tinea incognito?
The morphology deviates markedly from classic tinea:
- Minimal scaling or erythema, lacking annular configuration.
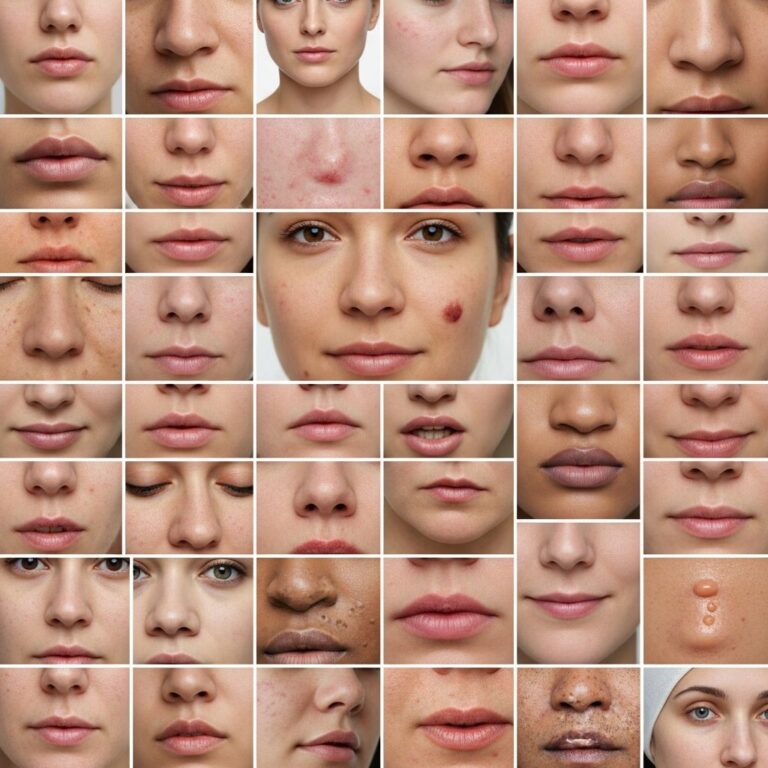
- Diffuse erythematous plaques, papules, pustules, or nodules on face, trunk, limbs, or flexures.
- Facial involvement resembling rosacea, lupus erythematosus, or granuloma faciale.
- Leg lesions mimicking cellulitis, granuloma annulare, or pretibial myxoedema.
Long-term steroid use induces secondary changes like telangiectasia, skin atrophy, striae, steroid acne, perioral dermatitis, or rosacea-like features. Abrupt steroid cessation triggers rebound inflammation with intense scaling and erythema at active borders. Extensive cases may show follicular involvement or kerion-like reactions. Dermoscopy reveals dotted vessels, peripheral white scales, and ‘moth-eaten’ borders post-steroid withdrawal.
Diagnosis of tinea incognito
Diagnosis is clinical-historical, supported by mycology:
- History of steroid/immunosuppressant use and poor response with rebound.
- Examination for subtle scaly, advancing edges.
Skin scrapings from the periphery, taken 3–7 days post-steroid cessation, undergo KOH microscopy (10–40%) revealing branched hyphae. Fungal culture identifies species and assesses resistance. Histopathology shows spongiosis, parakeratosis, and hyphae in stratum corneum; PAS stain confirms fungi. Advanced tools like PCR, MALDI-TOF-MS, or confocal microscopy offer higher sensitivity but are not routine. Dermoscopy aids suspicion with scales and vessels. Differential includes eczema, psoriasis, lichen simplex, granulomatous diseases, and bacterial infections.
What is the treatment for tinea incognito?
Key steps:
- Discontinue steroids/immunosuppressants immediately; use bland emollients or antipruritics for withdrawal symptoms.
- Topical antifungals for localized disease: terbinafine, azoles (clotrimazole, miconazole, luliconazole, econazole) twice daily for 2–4 weeks. Avoid steroid-antifungal combos due to persistent steroid effects.
- Oral antifungals for extensive, facial, or resistant cases: terbinafine 250 mg/day (4 weeks), itraconazole 200 mg/day (1–4 weeks), fluconazole 150–400 mg/week. Monitor LFTs for prolonged therapy.
Continue treatment 1–2 weeks post-clearance. Resistance (e.g., terbinafine-resistant T. indotineae) may necessitate culture-guided therapy.
What is the outcome of tinea incognito?
With prompt discontinuation of steroids and antifungals, most resolve in 2–8 weeks without scarring. Delays lead to dissemination, resistance, and chronicity. Secondary atrophy or telangiectasia from steroids may persist. Recurrence is common without prevention. Patient education on steroid misuse is vital.
How can tinea incognito be prevented?
- Avoid self-medicating with topical steroids; seek dermatological advice for persistent rashes.
- Use antifungals empirically if tinea suspected before steroids.
- Maintain hygiene: loose cotton clothing, hot water laundry, ironing, no sharing items.
- Perform KOH in steroid candidates, especially face/legs.
Frequently Asked Questions
Can tinea incognito affect the face?
Yes, facial tinea incognito often mimics rosacea or eczema due to common steroid application there.
Is oral antifungal always needed?
No, topical suffices for limited lesions, but oral is required for extensive or steroid-heavy cases.
How long after stopping steroids for diagnosis?
Wait 3–7 days for scrapings to allow fungal visibility.
Does it scar?
Rarely, unless secondary bacterial infection; steroid atrophy may linger.
Is it contagious?
Yes, via fomites or contact; prevent spread with hygiene.
References
- Tinea incognito — Cleveland Clinic Journal of Medicine. 2024-05-01. https://www.ccjm.org/content/92/5/271
- Descriptive review of Tinea incognito — Dove Medical Press (CCID). 2023-10-15. https://www.dovepress.com/tinea-incognito-peer-reviewed-fulltext-article-CCID
- Tinea incognito — DermNet NZ. 2024-01-10. https://dermnetnz.org/topics/tinea-incognito
- Tinea Incognito: Pink Patches on the Hip and Buttock — Dermatology Advisor. 2023-08-20. https://www.dermatologyadvisor.com/ddi/tinea-incognito/
- Tinea Incognito: Challenges in Diagnosis and Management — PMC/NCBI (PMC11172699). 2024-06-12. https://pmc.ncbi.nlm.nih.gov/articles/PMC11172699/
Similar Articles






Read full bio of Sneha Tete