Tungiasis: Complete Guide To Symptoms, Treatment And Prevention
Comprehensive guide to tungiasis: causes, symptoms, complications, treatment, and prevention of this neglected tropical skin infestation.

What is tungiasis?
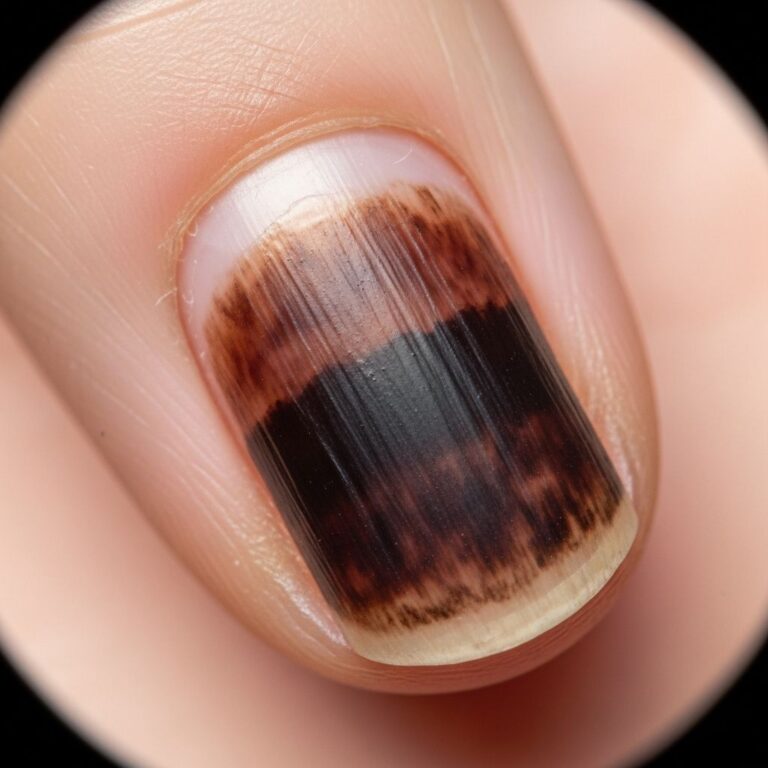
Tungiasis is a cutaneous parasitosis resulting from infestation by the female sand flea Tunga penetrans (Linnaeus, 1758; Siphonaptera, Tungidae) or related species such as Tunga trimamillata. Also known as chigoe flea, jigger, bicho de pie (bug of the foot), nigua, or sand flea, it causes a characteristic lesion described as a white patch with a central black dot. This neglected tropical disease predominantly affects the feet, leading to pain, itching, and potential severe complications like secondary bacterial infections.
The condition was first documented in the 1500s among crew members of Christopher Columbus shipwrecked on Haiti, where the fleas burrowed into their skin. Today, it impacts over 20 million people globally, especially in impoverished rural communities.
Who gets tungiasis?
Tungiasis primarily affects individuals in tropical and subtropical regions, including parts of Africa, Latin America, the Caribbean, India, and Pakistan. High-risk groups include:
- Poor rural populations and shanty town residents who walk barefoot.
- Children aged 5–14 years, particularly boys, and the elderly.
- People in contact with infested animals like pigs, cows, dogs, cats, and rats.
- Travelers to endemic areas without proper footwear.
Prevalence can reach 80% in disadvantaged children in endemic zones. Indoor transmission occurs in some settings, enabling year-round infestation.
Causes
The female T. penetrans flea, measuring less than 1 mm, burrows into the epidermis of warm-blooded hosts (humans and animals) to feed on blood and lay eggs. Despite myths, these fleas have limited jumping ability and do not leap; they attach via direct ground contact.
Endemic in warm, dry sandy soils of beaches, stables, and farms, fleas thrive in resource-poor environments. Zoonotic transmission links humans to animal reservoirs.
Life cycle of the flea
The flea life cycle includes on-host and off-host phases.
- Off-host: Eggs hatch into larvae in soil, feeding on organic matter before pupating.
- On-host: Impregnated females bite and burrow into the stratum corneum, advancing to the dermis. They hypertrophy, reaching 4–10 mm, with the posterior abdomen exposed as a black dot for breathing and egg expulsion.
- The flea produces up to 100–200 eggs over 1–6 weeks, which exit via the lesion to contaminate soil. It dies and sloughs off with shed skin.
Full cycle completes indoors in some areas.
Clinical features
Lesions appear as punctate ulcers or white patches (4–10 mm) with a central black dot (flea’s abdomen). Common sites: periungual toes, soles, heels (90% of cases). Other areas: hands, elbows, knees, genitalia, scalp.
| Stage | Description |
|---|---|
| Penetration | Early inflammatory papule. |
| Avulsion | Exposed flea with egg extrusion. |
| Excretion | Viable eggs expelled. |
| Debris | Dead flea remnants, suppuration. |
Symptoms: intense pruritus, pain, swelling. Multiple lesions cause walking impairment.
Complications
Untreated tungiasis leads to:
- Secondary infections: Cellulitis, abscess, bacteraemia (common), tetanus, gas gangrene, necrotising fasciitis (rare).
- Chronic morbidity: Nail loss, toe deformation, fissures, lymphangitis.
- Systemic risks: Sepsis in heavy infestations.
Unsafe self-removal exacerbates infections.
Diagnosis
Clinical: characteristic lesions suffice in endemic areas. Dermoscopy reveals the flea. Biopsy rarely needed. Differential: myiasis, tick bite, plantar warts.
Management
Often self-limiting (flea dies in 2 weeks). Symptomatic relief:
- Topical: petroleum jelly occlusion, potassium permanganate soaks.
- Neem-coconut oil mixture effective for pain/itch relief vs. KMnO4.
- Sterile surgical excision under magnification for viable fleas.
- Antibiotics for infections.
Avoid unsterile extraction.
Prevention
- Wear closed-toe shoes, socks, long pants in endemic areas.
- Apply plant-based repellents (e.g., Zanzarin®).
- Insecticide soil spraying (malathion).
- Hygiene, animal deinfestation.
History and epidemiology
Originating in the Americas, spread via slave trade. Endemic in sub-Saharan Africa (highest burden), Americas gaps in data. Poverty, barefoot walking key risk factors.
Frequently Asked Questions
What is tungiasis?
A skin infestation by burrowing female sand fleas causing painful lesions.
Where is tungiasis found?
Tropical/subtropical regions: Africa, Latin America, Caribbean.
How do you get tungiasis?
Direct contact with soil or infested animals while barefoot.
Does it go away on its own?
Yes, typically within 2–6 weeks as flea dies.
Can tungiasis cause serious problems?
Yes, secondary infections like tetanus or sepsis.
How is it treated?
Surgical removal, topical treatments, antibiotics if infected.
How can I prevent it while traveling?
Wear shoes, use repellents.
References
- Efficacy of a mixture of neem seed oil (Azadirachta indica) and coconut oil (Cocos nucifera) for topical treatment of tungiasis. A randomized controlled, proof-of-principle study — Feldmeier H et al. PLOS Negl Trop Dis. 2020-02-10. https://journals.plos.org/plosntds/article?id=10.1371/journal.pntd.0007822
- Tungiasis — DermNet NZ. 2008 (updated). https://dermnetnz.org/topics/tungiasis
- Myth or truth: investigation of the jumping ability of Tunga penetrans — Heukelbach J et al. PMC. 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10784774/
- Tungiasis: Causes, Symptoms, Removal & Treatment — Cleveland Clinic. 2023 (updated). https://my.clevelandclinic.org/health/diseases/24162-tungiasis
- Current status of the knowledge on the epidemiology of tungiasis in the Americas — Sanches F et al. Rev Panam Salud Publica. 2022. https://www.scielosp.org/article/rpsp/2022.v46/e124/en/
Similar Articles






Read full bio of medha deb