Steatocystoma Multiplex: Causes, Symptoms, and Treatment
Complete guide to steatocystoma multiplex: understanding this rare inherited skin disorder.

Steatocystoma Multiplex: A Complete Overview
Steatocystoma multiplex (SM), also known as steatocystomatosis, sebocystomatosis, or epidermal polycystic disease, is a rare benign intradermal true sebaceous cyst disorder affecting multiple areas of the body. This uncommon inherited skin condition results from hamartomatous malformation of the pilosebaceous duct junction, the area where hair follicles and sebaceous glands meet. The condition typically develops during adolescence or early adulthood and is characterized by the progressive appearance of numerous small, firm cystic nodules across various body locations. Understanding this condition is essential for proper diagnosis and management, as it can significantly impact quality of life and may be confused with other dermatological conditions.
Classification and Types of Steatocystoma Multiplex
Steatocystoma multiplex presents in several distinct clinical variants, each with unique characteristics and presentations. The classification system includes:
- Localized type: Limited to specific body regions, typically the chest or axillae
- Generalized type: Widespread distribution across multiple body areas
- Facial type: Predominantly affecting facial skin
- Flexural type: Concentrated in body creases and folds
- Acral type: Affecting extremities, hands, and feet
- Syndromal type: Associated with other systemic or genetic features
- Suppurative type: Characterized by inflammation and infection of lesions
Additionally, atypical presentations include giant steatocystoma multiplex, linear patterns, palatal involvement, and extensive calcification. The solitary counterpart to steatocystoma multiplex is known as steatocystoma simplex, which represents a single isolated lesion rather than multiple cysts.
Clinical Features and Presentation
Steatocystoma multiplex typically manifests as multiple, asymptomatic, round, smooth, firm, and mobile cystic papules and nodules of varying sizes, ranging from a few millimeters to several centimeters in diameter. The lesions appear uniform in presentation but can vary in color and depth. Superficial lesions typically appear yellowish due to their sebum content, while deeper lesions tend to be skin-colored and less visible on the surface.
The lesions are usually soft to firm, discretely margined, and flat-topped when examined clinically. They commonly appear during adolescence and progressively increase in number and size over years of development. The most common locations for these cysts include:
- Anterior chest wall
- Axillae (underarms)
- Epigastrium (upper abdomen)
- Groin region
- Neck area
- Proximal parts of extremities and upper arms
- Scrotum
Less frequently, steatocystoma multiplex may involve the back, abdomen, and external genitalia, while facial and scalp involvement is rare. The lesions are typically asymptomatic, though individual cysts may occasionally discharge oily material when incised or rupture.
Genetic and Hereditary Factors
Steatocystoma multiplex is inherited as an autosomal dominant trait, meaning only one mutated gene copy from either parent is necessary for the condition to develop. Genetic changes in the KRT17 gene located on chromosome 17q21.2 have been identified as the underlying cause of this condition. Approximately 40-60% of patients report a relevant family history, though sporadic cases that develop without familial predisposition have also been documented.
Both sexes are equally affected by the condition, though some literature suggests a slightly higher prevalence in males. The autosomal dominant inheritance pattern means that affected individuals have a 50% chance of passing the condition to their offspring. However, variable expressivity can occur, resulting in different severity levels and manifestations among family members carrying the same genetic mutation.
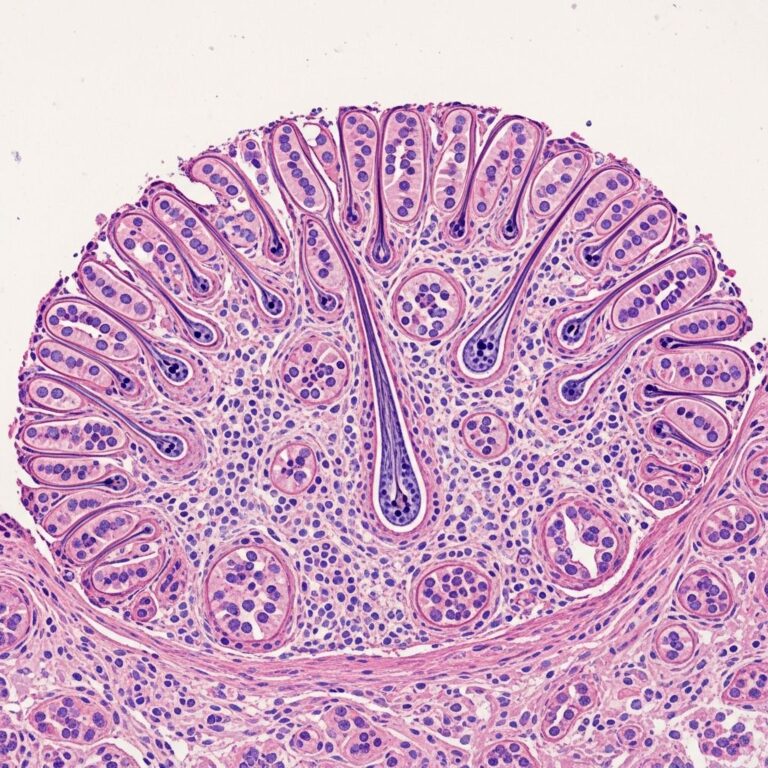
Pathophysiology and Histopathology
The underlying mechanism of steatocystoma multiplex involves a defect at the pilosebaceous duct junction, leading to abnormal cyst formation within the skin layers. Histopathologically, the lesions consist of multiple round cysts located in the mid and deep dermis, with cyst walls composed of three to five layers of squamous epithelium. These cyst walls are lined with flattened sebaceous glands and feature undulating acellular eosinophilic cuticles characteristic of sebaceous differentiation.
The cysts contain keratin-filled material and numerous transversely or obliquely cut vellus hair shafts within their cavities. This unique histological composition distinguishes steatocystoma multiplex from other cystic lesions and is essential for definitive diagnosis. The sebaceous content gives the cysts their characteristic oily nature and yellowish appearance when expressed.
Complications and Associated Conditions
While steatocystoma multiplex is generally benign, complications can develop during its natural course. The condition can transform into steatocystoma multiplex suppurativum (SMS), also known as steatocystoma multiplex conglobatum, at any point during its progression. This variant is characterized by inflamed, ruptured, and draining cysts that may result in scarring and secondary bacterial infection.
Key complications include:
- Cyst rupture and drainage of sebaceous material
- Associated pain and pruritus (itching)
- Pyrexia (fever) in some cases
- Secondary bacterial infections leading to abscess formation
- Malodorous discharge from infected lesions
- Scarring from repeated inflammation and rupture
- Features overlapping with hidradenitis suppurativa
Rare presentations have been documented, including vulvar steatocystoma multiplex affecting sexual activity in women and scalp involvement with concurrent alopecia secondary to trichotillomania. Cases of multiple steatocystoma multiplex have been reported in patients undergoing immunosuppressive treatment with agents such as ustekinumab.
Diagnosis and Differential Diagnosis
Diagnosis of steatocystoma multiplex is usually established clinically based on patient history, physical examination findings, and the characteristic presentation of multiple cystic lesions in typical locations. However, biopsy and histopathological examination may be required for definitive confirmation, particularly in atypical presentations or when clinical diagnosis is uncertain.
Steatocystoma multiplex can be confused with several other dermatological conditions, making differential diagnosis important:
- Milia and milia-like cysts
- Epidermal inclusion cysts and sebaceous cysts
- Lipomas and fat necrosis
- Dermoids
- Cysts of acne vulgaris
- Galactoceles (in breast tissue)
Imaging studies, including sonography and mammography, may be utilized in specific cases to characterize lesions and rule out other conditions. Ultrasound typically reveals multiple relatively well-circumscribed and homogeneous lesions that are hypoechoic with posterior enhancement, confined to the dermis. Most lesions (83.3%) appear as hypoechoic on ultrasound, with posterior acoustic enhancement present in approximately 77.8% of nodules.
Treatment Options
Long-term management of steatocystoma multiplex is challenging, and spontaneous resolution is not expected to occur. Multiple therapeutic approaches exist, each with varying degrees of efficacy and cosmetic outcomes. Treatment selection depends on the extent of disease, patient preferences, and desired cosmetic results.
Surgical Removal: This remains the most definitive treatment option, involving direct excision of individual lesions or affected skin regions. Surgical approaches provide permanent removal but may result in scarring, particularly when multiple lesions are treated.
Needle Aspiration: This minimally invasive technique involves puncturing cysts and extracting their sebaceous contents. However, cysts frequently recur following aspiration, limiting its long-term effectiveness as a sole treatment approach.
Cryotherapy: Freezing individual lesions with liquid nitrogen can be effective for select cysts but may require multiple treatment sessions and carries risks of hypopigmentation or hyperpigmentation.
Isotretinoin (Accutane): This systemic retinoid therapy has shown promise in managing steatocystoma multiplex by reducing sebaceous gland activity and potentially preventing new cyst formation. However, its use requires careful monitoring due to potential systemic side effects and teratogenic risks in pregnant individuals.
CO2 Laser Treatment: Carbon dioxide laser therapy offers excellent cosmetic outcomes for treating multiple lesions with controlled ablation of affected skin areas. This approach provides precise tissue removal and can address large treatment areas effectively.
Psychosocial Impact and Adolescent Development
For adolescents, steatocystoma multiplex can have significant developmental and psychological impact. The appearance of numerous visible skin lesions during a critical developmental period can affect self-esteem, body image, and social interactions. Early diagnosis and discussion of available treatment options are essential for supporting affected adolescents through this challenging period.
The progressive nature of the condition, with lesions increasing in number and size over time, may contribute to anxiety and concern about cosmetic appearance. Educational interventions helping patients understand the benign nature of the condition and the available management strategies can improve psychological outcomes and quality of life.
Prognosis and Long-term Management
Steatocystoma multiplex is a lifelong condition without spontaneous resolution expected. The cysts typically persist and may continue to increase in number throughout life. Regular dermatological follow-up is recommended to monitor lesion progression, assess for complications, and discuss treatment options. Patients should be educated about the benign nature of the condition and the importance of avoiding self-manipulation or attempted drainage of lesions, which can lead to infection and scarring.
Management strategies should be individualized based on patient concerns, lesion burden, and desired cosmetic outcomes. For asymptomatic, stable lesions that are not bothersome to the patient, observation without active treatment may be appropriate. For patients seeking cosmetic improvement or experiencing complications, various treatment modalities can be considered.
Frequently Asked Questions
Q: Is steatocystoma multiplex contagious?
A: No, steatocystoma multiplex is not contagious. It is a genetic, inherited condition resulting from a defect in the pilosebaceous duct junction. The condition cannot be transmitted from person to person through contact.
Q: Can steatocystoma multiplex become cancerous?
A: No, steatocystoma multiplex is a benign condition and does not develop into cancer. However, individual cysts can become infected, leading to complications such as abscess formation and scarring.
Q: At what age does steatocystoma multiplex typically appear?
A: Steatocystoma multiplex typically appears during adolescence or young adulthood. Lesions progressively increase in number and size over years, though the exact onset and progression rate can vary among individuals.
Q: If one parent has steatocystoma multiplex, will their children develop it?
A: Since steatocystoma multiplex is inherited as an autosomal dominant trait, children of affected parents have a 50% chance of inheriting the condition. However, genetic counseling can provide personalized risk assessment.
Q: Are there any preventive measures to avoid developing steatocystoma multiplex?
A: Since steatocystoma multiplex is a genetic condition, it cannot be prevented. However, patients can avoid manipulating or squeezing lesions to prevent infection and scarring complications.
Q: What is the difference between steatocystoma multiplex and steatocystoma simplex?
A: Steatocystoma simplex is a solitary lesion counterpart to steatocystoma multiplex. While steatocystoma multiplex involves multiple cysts, steatocystoma simplex consists of a single isolated sebaceous cyst with similar histological characteristics.
References
- Steatocystoma Multiplex — PubMed Central, National Institutes of Health. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC10810380/
- Steatocystoma Multiplex: Mammographic and Sonographic Features — American Journal of Roentgenology. 2003. https://ajronline.org/doi/10.2214/ajr.180.1.1800271
- Steatocystoma Multiplex — MalaCards Database. 2024. https://www.malacards.org/card/steatocystoma_multiplex
- Steatocystoma Multiplex — VisualDx Clinical Decision Support. 2024. https://www.visualdx.com/visualdx/diagnosis/?moduleId=101&diagnosisId=52341
- Steatocystoma Multiplex — JAMA Dermatology. 2003. https://jamanetwork.com/journals/jamadermatology/fullarticle/536389
- Steatocystoma Multiplex: Case Report and Review of Treatment — DermSquared Journal of Clinical Dermatology. 2020. https://skin.dermsquared.com/skin/article/view/51
- Steatocystoma Multiplex and Adolescent Development — Journal of Nursing Education. 2013. https://nursing.ceconnection.com/ovidfiles/01412499-201303000-00004.pdf
Similar Articles






Read full bio of Sneha Tete